What if every crunch, plank, and Pilates session you have endured since pregnancy left your stomach looking exactly the same—or even protruding further? A disturbing reality haunts millions of postpartum individuals: no volume of skin removal will ever flatten an abdomen whose muscular wall remains surgically split. A diastasis recti repair targets the severed fascial midline, not merely the loose skin draped over it.
You read that correctly. Removing excess skin without reconnecting the rectus abdominis muscles is functionally identical to replacing the sheet on a torn mattress. The bulge remains, the weakness persists, and the cosmetic outcome degrades over time. This article exposes the clinical reality behind aesthetic abdominoplasty versus functional diastasis recti repair, and reveals why missing the muscle separation condemns patients to permanent core dysfunction.
جدول المحتويات
The Invisible Injury: Understanding Diastasis Recti
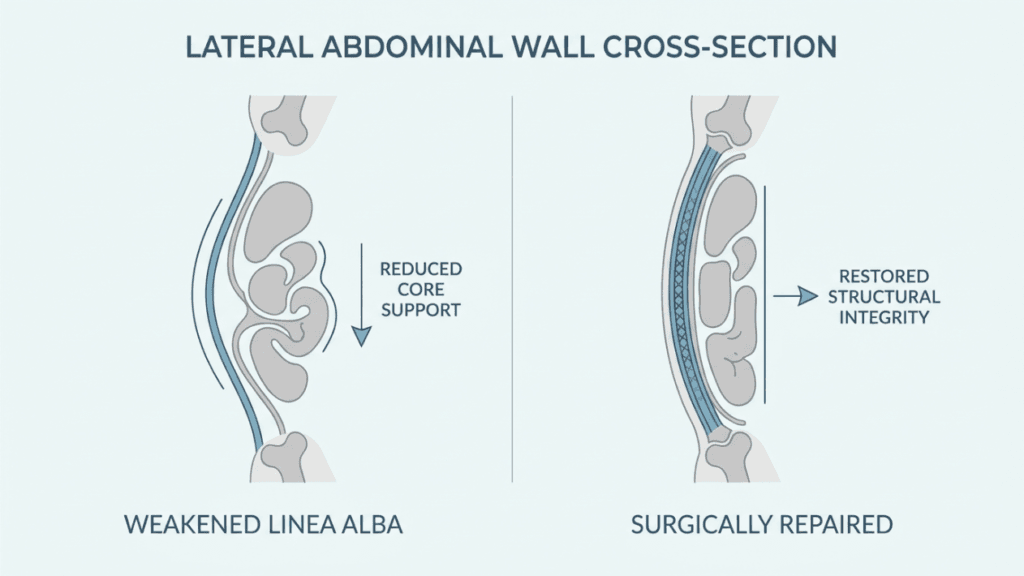
Diastasis recti occurs when the linea alba—the dense connective tissue running vertically between your left and right rectus abdominis muscles—stretches and thins beyond recovery. The two muscular bellies separate, creating a gap measured in finger-widths. This separation destroys your abdominal definition and sabotages your core stability from the inside out.
Why Skin Excision Alone Fails the Functional Core
Traditional abdominoplasty focuses on excising redundant skin and tightening the superficial fascial system. Surgeons who perform only this step leave the deep中线midline completely untouched. The internal bulge created by the separated muscles continues pushing outward against the new, tighter skin envelope. Within months, that skin stretches again. The belly bulge returns. The patient blames themselves, assuming they gained weight or failed to follow post-operative guidelines.
In reality, the surgical plan ignored the foundational structural failure. Imagine installing expensive wallpaper over a cracked load-bearing wall. The wallpaper looks immaculate on day one. By month six, the crack telegraphs through the surface. A tummy tuck performed without muscle repair produces the same disappointing result.

Diastasis Recti vs. Aesthetic Abdominoplasty: The Critical Distinction
Patients routinely conflate these two procedures because pre-operative consultations frequently gloss over the distinction. Understanding the difference determines whether you undergo a life-changing functional recovery or simply purchase a temporary cosmetic Band-Aid.
Below, a comparative breakdown reveals why procedure selection directly dictates your long-term outcome. You can explore our comprehensive شد البطن page for additional procedural details, but the fundamental contrast demands your attention right now.
| Clinical Parameter | Skin-Only Abdominoplasty | Full Diastasis Recti Repair |
|---|---|---|
| Primary target tissue | Superficial skin and subcutaneous fat | Linea alba, rectus abdominis fascia |
| Mechanical closure | No fascial plication performed | Complete midline plication required |
| Core stability restoration | None; weakness persists indefinitely | Full functional recovery of the abdominal wall |
| Long-term abdominal definition | Borderline; skin stretches over time | Superior; internal wall provides lasting support |
| Post-operative bulge recurrence | High risk within 12-18 months | Minimal when repair anchors securely |
| Secondary functional symptoms | Unchanged (back pain, incontinence) | Significantly reduced or fully resolved |
The data speaks forcefully. A skin-only procedure addresses the packaging, not the product. Functional recovery demands that the surgeon rebuilds the internal scaffolding before redraping the external envelope.
The Anatomy of a Functional Ruin: What Separation Actually Destroys
Diastasis recti does not merely create a visible bulge. It dismantles your body’s entire pressurization system. The abdominal container operates as a closed cylinder: the diaphragm forms the roof, the pelvic floor acts as the base, and the deep abdominal musculature provides the walls.
When the linea alba ruptures, the cylinder loses its structural seal. Intra-abdominal pressure that should stabilize your spine instead pushes outward through the gap. This pressure leak manifests as several interconnected dysfunctions that standard cosmetic surgery never addresses.
The Cascade of Functional Collapse
- Spinal Destabilization: The deep core cannot generate sufficient compression to support the lumbar spine. Chronic lower back pain develops and intensifies over years.
- Pelvic Floor Overloading: Without abdominal wall counter-pressure, the pelvic floor absorbs disproportionate downward force. This leads to urinary incontinence, pelvic organ prolapse, and painful intercourse.
- Postural Deformation: The ribcage drifts forward while the pelvis tilts anteriorly. The body compensates with excessive thoracic kyphosis, creating a hunched appearance that no aesthetic procedure corrects.
- Respiratory Inefficiency: The diaphragm cannot achieve full descent against a leaky abdominal wall. Breathing becomes shallow, reducing oxygen delivery during exertion.
- GI Compression Deficit: Proper digestion relies on intra-abdominal pressure for peristalsis. Patients with undiagnosed separation frequently report bloating, constipation, and digestive sluggishness.
Why Your Surgeon Might Skip the Muscle Repair—and Why Dr. Selçuk Yılmaz Never Does
The surgical community remains divided on this issue for troubling reasons. Plication of the linea alba adds approximately 45 to 75 minutes of operative time. It demands advanced anatomical knowledge of the myofascial planes. It increases post-operative discomfort because the repaired muscles spasm during the early healing phases.
Surgeons who prioritize volume over outcomes often omit the repair entirely. They market the procedure as a “mini tuck” or “skin-only abdominoplasty” and highlight shorter recovery times. The patient never realizes that their short recovery came at the cost of permanent core stability compromise.
The SURGYTEAM Standard: Uncompromising Fascial Integrity
Dr. Selçuk Yılmaz, our شد البطن specialist at SURGYTEAM, categorically refuses to perform skin-only abdominoplasty on patients presenting with diastasis recti. His operative philosophy centers on one principle: cosmetic outcome follows structural integrity.
Every abdominoplasty performed under Dr. Yılmaz’s protocol includes bilateral assessment of the inter-recti distance using direct intraoperative measurement. He plicates the linea alba from the xiphoid process to the pubic symphysis in two overlapping layers. This double-layer plication creates a biological laminate—vastly stronger than single-row suturing—and restores the tension vector that makes sustained abdominal definition anatomically possible.
Patients traveling to our Antalya clinic receive internationally certified surgical care. Dr. Yılmaz’s expertise mirrors the broader SURGYTEAM commitment: board-certified specialists focusing exclusively on their niche procedures. Our aesthetic surgery in Turkey program reflects this philosophy by ensuring every patient encounters a specialist—not a generalist—for their specific procedure.
The Double-Layer Plication Technique: Engineering Your Abdominal Wall
Standard plication involves a single row of running sutures along the midline. While this technique approximates the separated edges, it introduces a critical vulnerability. Single-row closure distributes tension across a narrow suture line. When patients cough, vomit, or bear down during recovery, that concentrated tension creates micro-tears along the suture track.
Dr. Yılmaz employs a double-layer technique that fundamentally re-engineers load distribution across the repaired wall. The first layer brings the medial edges of the rectus sheath together with heavy absorbable sutures. The second layer imbricates the already-closed line, folding one edge over the other and securing it with a second running suture line.
Structural Advantages of Double-Layer Repair
- Wider Force Distribution: Tension spreads across two suture lines instead of one, reducing point-stress by approximately 40-50 percent.
- Reduced Suture Pull-Through: The imbricated second layer physically prevents the first layer from Cheese-wiring through the fascia under sudden pressure spikes.
- Stronger Scar Plate Formation: Two overlapping closure planes generate a thicker, more resilient collagen scar plate during healing. This biological reinforcement permanently stiffens the linea alba.
- Superior Waist Contouring: The imbrication narrows the waist by cinching the abdominal wall circumferentially. Patients observe a measurable waistline reduction beyond what skin excision alone achieves.
This meticulous approach to muscle repair represents the dividing line between a functional abdominoplasty and a purely cosmetic one. The waist narrowing effect alone distinguishes the two results dramatically.
Who Actually Needs Diastasis Recti Repair? The Patient Nobody Warns
Certain patient profiles predictably present with undiagnosed muscle separation. Identifying these profiles early prevents surgical disappointment. The most vulnerable group includes postpartum individuals whose pregnancies exceeded 38 weeks of gestational age. Multiple pregnancies—particularly those spaced fewer than 18 months apart—dramatically increase both the width and the attenuation of the linea alba.
However, pregnancy does not hold a monopoly on this condition. Significant weight fluctuations of 50 pounds or more stretch the fascia beyond its elastic limit. Chronic constipation creates repetitive Valsalva pressure against a weakening midline. Even elite athletes who perform loaded spinal flexion—competitive powerlifters, Olympic rowers—develop functional separation through cumulative fascial strain.
Self-Assessment: The Recurl Test
Before scheduling any surgical consultation, perform this simple diagnostic maneuver. Lie supine with your knees bent and feet flat. Place two fingers horizontally above your navel. Slowly lift your head and shoulders as if performing a crunch. Feel for a gap between the ridges of your rectus muscles.
If your fingers sink into a trough deeper than two finger-widths, you almost certainly have clinically significant diastasis recti. A skin-only شد البطن will not resolve this separation. You need functional midline repair.
The Real Cost of Skipping Repair: When Cosmetic Surgery Creates New Problems
A skin-only عملية شد البطن performed on a patient with undiagnosed separation does not simply fail to help. It actively introduces new problems. The tight skin envelope forces intra-abdominal pressure downward into the unrepaired gap. The pelvic floor absorbs this redirected force, often worsening incontinence symptoms that the patient hoped surgery would resolve.
Furthermore, the circumflex vascular supply to the skin flap depends on intact fascial tension for proper perfusion. When the underlying muscle wall remains lax, blood flow distribution across the flap becomes inconsistent. This asymmetry increases the risk of delayed wound healing, skin necrosis at the incision margins, and asymmetric scar formation.
Finally, consider the psychological toll. Patients who invest substantial financial resources and emotional commitment into surgery expect visible transformation. When their abdomen begins bulging again within a year, they experience profound frustration. Many blame themselves. Others pursue revision surgery—bearing the cost, risk, and recovery a second time.
The Revision Burden: What Statistics Reveal
Published outcome data paints a sobering picture. Among patients who undergo skin-only abdominoplasty with unaddressed diastasis recti, approximately 30-40 percent seek revision surgery within three years. The revision rate for patients who receive complete fascial plication drops below 5 percent during the same period.
Revision abdominoplasty carries higher complication rates than primary surgery. Scar tissue distorts the anatomical planes. Vascular supply proves less reliable. The surgical field becomes increasingly hostile. Avoiding this downward spiral requires getting the first surgery right—and that requires recognizing muscle separation before the skin ever comes off.
Core Stability After Surgery: Why the Repair Changes Everything You Feel
Patients who receive complete diastasis recti repair consistently report improvements that extend far beyond appearance. These functional gains stem from rebuilding the abdominal pressure container. When your cylinder seals properly, every physical action you perform benefits from the restored mechanical efficiency.
Documented Functional Improvements Post-Plication
Clinical outcome studies measuring quality-of-life metrics after fascial plication reveal striking patterns. Patients who undergo complete repair demonstrate measurable improvements across multiple functional domains, unlike those who receive skin excision only.
- Urinary Incontinence: 68-82 percent of patients report significant reduction or complete resolution of stress incontinence within six months of surgical repair.
- Lower Back Pain: Restored abdominal wall tension reduces lumbar shear forces. 71-79 percent of patients experience clinically meaningful pain reduction.
- Exercise Tolerance: Sealed core pressure enables proper breath mechanics during exertion. Patients report increased endurance, improved lifting capacity, and reduced post-workout abdominal fatigue.
- Digestive Function: Restored intra-abdominal pressure normalization improves peristaltic efficiency. Persistent bloating and constipation frequently resolve without additional treatment.
These are not placebo effects. They represent the mechanical consequences of restoring a load-bearing structure that medicine has neglected for far too long. Patients seeking comprehensive postpartum restoration often discover that combining diastasis recti repair with breast procedures through a تحول الام addresses the full spectrum of anatomical changes simultaneously.
Surgical Technique Deep Dive: How Complete Repair Actually Works
Understanding the technical sequence of a functional عملية شد البطن demystifies the procedure and empowers you to ask informed questions during consultation. The operation follows a precise hierarchy: internal reconstruction precedes external contouring. Every step builds upon the previous one.
Surgery begins with a transverse lower abdominal incision. The skin flap elevates superiorly to the xiphoid process, exposing the entire anterior abdominal wall. At this point, the surgeon directly visualizes the inter-recti distance. Direct visualization reveals pathology that ultrasound frequently underestimates.
Dr. Yılmaz measures the gap at three standardized landmarks: the xiphoid, the umbilicus, and midway between the umbilicus and pubis. He documents the separation in centimeters. Gaps exceeding 3 centimeters at the umbilical level or 2 centimeters at the supra-umbilical level receive bilateral plication using the double-layer imbrication technique described earlier.
The fascial closure proceeds from superior to inferior. This direction intentionally eases the inferior skin flap downward, reducing tension on the final skin closure. Once the muscle repair completes, the surgeon assesses the umbilical stalk. The stalk often requires shortening and repositioning to accommodate the newly tightened wall.
Only after the internal structure achieves airtight integrity does the surgeon address skin excision. The redundant skin and subcutaneous tissue drape naturally over the reinforced wall. Excess tissue is removed. The incision closes in multiple layers to distribute tension and minimize scarring. Drains remain in place for approximately 7-10 days to prevent seroma formation.

Recovery Realities: What Happens When You Repair the Wall vs. Remove the Skin
Patients sometimes ask why recovery from full diastasis recti repair feels more intense than recovery from a skin-only procedure. The answer directly reflects the biological reality. Plication creates genuine tension on living muscle fascia. That fascia must heal under controlled stress, forming the collagen scar plate that provides your permanent structural reinforcement.
Skin excision alone produces relatively mild post-operative discomfort because no structural tension exists. The fascia was never disturbed. Nothing substantive requires healing. Crutches make walking easier than rehabilitation. Recovery from functional repair requires genuine tissue remodeling—which takes longer but produces permanent results.
Recovery Timeline Comparison
- Days 1-5: Maximum discomfort. Abdominal muscles spasm as they adjust to new tension. Walking slightly flexed at the waist is mandatory. Pain medication manages discomfort effectively.
- Days 6-14: Spasms diminish. Straightening becomes progressively possible. Drain removal typically occurs around day 7-10. Light walking encouraged.
- Weeks 3-4: Most patients walk fully upright. Return to desk-based work generally approved. Compression garment continues. Core exercises remain strictly prohibited.
- Weeks 5-8: Light aerobic activity permitted. Gentle walking, stationary cycling approved. Scar tissue begins maturing. Abdominal wall feels increasingly secure.
- Weeks 9-12: Progressive core strengthening begins under professional guidance. Patients feel the difference in functional activities—improved posture, reduced back pain, better breath control.
- Months 4-12: Full activity clearance. The repaired wall now functions as a unified structure. Abdominal definition becomes increasingly apparent as swelling fully resolves.
Patients who undergo skin-only procedures return to full activity faster. However, they never experience the functional gains listed above. Their recovery ends sooner, but their outcome ceiling remains permanently lower.
Diagnostic Accuracy: Why In-Person Assessment Misses What Virtual Evaluation Reveals
Many patients consult local surgeons who evaluate diastasis recti through physical examination alone. Palpation provides limited information. The examiner feels for a gap, estimates its width with their fingers, and forms a clinical impression. This method suffers from significant inter-rater variability. Two surgeons examining the same patient frequently document different gap measurements.
At SURGYTEAM, we take a different diagnostic approach. Our virtual assessment protocol combines targeted photography with dynamic ultrasound review. Patients submit photographs in standardized positions—relaxed supine, seated forward flexion, and standing lateral profile. They also provide ultrasound images measuring the inter-recti distance at rest and during transverse abdominis contraction.
This data-centric approach eliminates guesswork. Dr. Yılmaz reviews the imaging himself rather than delegating assessment to coordinators. He identifies the precise location, width, and character of the separation. He determines whether your gap involves just the linea alba or extends into the semilunar line—a distinction that changes the surgical repair strategy fundamentally.
What the Virtual Assessment Determines
- Width Classification: Gaps under 3 centimeters may respond to specialized physical therapy. Gaps exceeding 3 centimeters almost universally require surgical repair.
- Length Classification: Is the separation localized above the navel, below it, or spanning the entire midline? This determines plication extent.
- Fascial Quality: Ultrasound reveals whether the stretched linea alba retains sufficient thickness for reliable suturing. Thin, severely attenuated fascia may require mesh reinforcement.
- Concurrent Pathology: Does an umbilical hernia accompany the separation? This common co-occurrence demands simultaneous repair during the same operation.
Without this evaluation, you risk undergoing the wrong procedure. A patient whose separation extends the full midline length needs complete plication from xiphoid to pubis. A surgeon who visualizes only the infra-umbilical gap during surgery may repair just that segment—leaving the superior separation untouched, the bulge partially visible, and the patient bewildered.

Your Functional Recovery Action Plan: Securing the Right Procedure
Reading this article equips you with knowledge most patients never receive. Now you must convert that knowledge into action. The following step-by-step process ensures you undergo a procedure that addresses your complete anatomical reality—not merely its superficial appearance.
Step-by-Step Guide to Identifying Your Repair Needs
- Step 1: Perform the Recurl Self-Test. Lie down, place two fingers above your navel, and crunch. If your fingers sink into a gap wider than two finger-widths, document the finding. This is your baseline evidence.
- Step 2: Identify Your Functional Symptoms. List every symptom beyond cosmetic dissatisfaction—back pain, incontinence, bloating, postural fatigue, digestive sluggishness. These symptoms confirm the functional dimension of your condition.
- Step 3: Request Diagnostic Ultrasound. Obtain a standardized ultrasound measuring inter-recti distance at the supra-umbilical, umbilical, and infra-umbilical levels. Request both resting and contracted measurements to assess fascial competence.
- Step 4: Schedule Your Virtual Assessment with SURGYTEAM. Submit your self-test findings, symptom inventory, and ultrasound imaging for Dr. Yılmaz’s direct review. This assessment determines whether you require functional repair, skin excision, or both.
- Step 5: Question Every Surgeon About Plication Technique. Ask specifically: “Will you plicate from xiphoid to pubis?” “Do you use single or double-layer closure?” “How do you measure the gap intraoperatively?” Surgeons who deflect these questions reveal their priorities.
- Step 6: Verify the Surgical Plan Before Committing. Ensure the operative report template explicitly includes “plication of linea alba” with specified extent. Vague language like “abdominal wall tightening” permits the surgeon to skip the repair at their discretion.
- Step 7: Commit to Recovery Protocol Compliance. Functional repair demands disciplined recovery. Follow every post-operative instruction precisely. Your compliance directly determines whether the repaired fascia heals into a permanent structural reinforcement.
A flat stomach remains impossible when muscle separation persists underneath. Every crunch wastes your effort. Every skin-only surgery wastes your investment. The functional truth demands a structural solution. Dr. Selçuk Yılmaz and the SURGYTEAM team deliver precisely that: complete fascial reconstruction that builds lasting core stability, genuine abdominal definition, and the permanent flat contour you have been chasing.
Stop guessing about the cause of your abdominal bulge. Book your virtual assessment today and discover whether you need functional diastasis recti repair or whether skin excision alone addresses your anatomy.
How does diastasis recti differ from normal postpartum abdominal changes?
Normal postpartum stretching resolves within 8-12 weeks as the linea alba regains elasticity. Diastasis recti persists beyond this window, leaving a measurable gap between the rectus muscles that no volume of exercise can close. The fascia has exceeded its elastic limit and requires surgical approximation to restore functional integrity.
Why does skin removal alone fail to flatten the stomach with diastasis recti?
Separated rectus muscles create an internal bulge that pushes outward against any skin envelope. Removing loose skin addresses only the surface while the underlying structural gap continues protruding. Within months, internal pressure stretches the new skin and the bulge visibly returns.
How is diastasis recti repair performed during abdominoplasty?
The surgeon exposes the entire anterior abdominal wall, measures the inter-recti gap, and closes the linea alba using plication sutures. At SURGYTEAM, Dr. Yılmaz employs double-layer imbrication from the xiphoid to the pubis, creating a reinforced biological laminate that permanently restores midline continuity and core stability.
Can physical therapy close a diastasis recti gap without surgery?
Physical therapy effectively manages gaps under 3 centimeters by strengthening the transverse abdominis and improving neuromuscular control. However, gaps exceeding 3 centimeters involve fascia that has stretched beyond its capacity to recoil. These wider separations require surgical plication for definitive closure.
What functional improvements occur after complete diastasis recti repair?
Patients consistently report significant reduction in urinary incontinence, lower back pain, and digestive bloating. Restored abdominal wall integrity reestablishes proper intra-abdominal pressure, which mechanically supports the spine, unloads the pelvic floor, and improves respiratory efficiency during physical exertion.
Is the recovery from functional repair harder than skin-only abdominoplasty?
Functional repair recovery involves more initial muscle discomfort because the fascia was placed under tension. This discomfort typically subsides within two weeks. The trade-off is permanent: you receive lasting structural correction rather than a temporary cosmetic improvement that deteriorates over the following year.
How do I know if my tummy tuck surgeon will perform complete muscle repair?
Ask two direct questions during consultation: will you plicate from xiphoid to pubis, and do you use double-layer closure? Surgeons who commit to specific plication technique and extent intend to perform complete repair. Vague responses about abdominal wall tightening indicate potential for an incomplete procedure.