That fox eye thread lift you walked out of the clinic smiling about last year? It is silently pulling your lateral canthal tendon apart — and within 36 months, no surgeon on Earth can undo it naturally. The barbed sutures buried beneath your temporal skin are not simply holding your eyelid in a lifted position. They are applying continuous, unrelenting upward tension to a tendon that was never engineered to carry that load, and that tendon is now detaching from your orbital rim one fiber at a time.
This is not speculation. This is canthal tethering — a documented ophthalmologic phenomenon that thread lift providers never mention during consultation. Canthal tethering describes the progressive stretching and eventual detachment of the lateral canthal tendon caused by persistent traction from thread-based lifts. Once that tendon separates from bone, your eyelid loses its structural anchor. Scleral show widens. Ectropion creeps in. And the only path back is a full canthal reconstruction — at four times the original procedure cost.
Table of Contents
Your Lateral Canthal Tendon: The Anchor Nobody Told You About
The lateral canthal tendon is not a cosmetic detail — it is the structural hinge of your entire eyelid mechanism. This fibrous band anchors the lateral commissure (the outer corner where your upper and lower eyelids meet) firmly to the Whitnall tubercle on the internal aspect of the orbital rim. Without this anchor, your eyelid cannot maintain its apposition against the globe. It cannot protect your cornea. It cannot blink properly.
Think of the lateral canthal tendon as the steel cable holding a suspension bridge to its concrete pillar. The tendon absorbs every micro-movement your eye makes — blinking, squinting, sleeping, rubbing. It handles thousands of cycles per day without complaint because it was designed to distribute force across a broad insertion point on bone. Thread lifts ignore this engineering entirely.
The Periorbital Anatomy Thread Providers Conveniently Skip
Understanding periorbital anatomy explains why thread lifts fail catastrophically in this region. The periorbital zone contains the thinnest skin on the human body — just 0.5mm over the eyelid. Beneath that paper-thin layer sit the orbicularis oculi muscle, the orbital septum, the lateral canthal tendon, and the lacrimal gland. Thread lifts bypass all of these structures blindly, inserting barbed polydioxanone or polypropylene sutures through a needle puncture and threading them into the superficial temporal fascia.
The problem crystallizes when you examine force vectors. A fox eye thread lift pulls the lateral canthus upward and outward at approximately 30 to 45 degrees. The lateral canthal tendon, however, inserts onto the orbital rim at roughly 10 degrees from horizontal. That angular mismatch means the thread is constantly trying to peel the tendon off bone like pulling tape off a wall — slowly, relentlessly, every single day.
Canthal Tethering: The Slow Detachment Nobody Diagnoses
Canthal tethering is not a sudden event. It is a slow, mechanical failure that unfolds over 18 to 36 months. Here is what happens beneath your skin while you admire your new cat-eye shape in the mirror.
Month 0 to 6: The Silent Stretch Phase
After thread insertion, the barbs engage the surrounding tissue. Initially, the threads grip the superficial temporal fascia and pull the lateral canthal angle upward. The result looks exactly like what the patient wanted — a swept, almond-shaped eye. But the lateral canthal tendon is already bearing abnormal tension. Collagen fibers within the tendon begin experiencing mechanical creep — a phenomenon where sustained loads cause tissue to elongate permanently beyond its elastic limit.
At this stage, the patient notices nothing wrong. The eyelid sits slightly higher. The canthal angle has migrated perhaps 2 to 3 millimeters. No doctor measures this. No patient complains. The damage accumulates silently.
Month 6 to 18: The Visible Drift Phase
As mechanical creep continues, the tendon insertion begins separating from the Whitnall tubercle. Patients start noticing changes: a slight widening of the white space between their iris and the outer corner of the eye. This is early scleral show. The lower eyelid begins losing its snug fit against the globe. Some patients report dryness, a gritty sensation, or excessive tearing because the punctum — the tiny drainage hole on the lower eyelid — is drifting away from its proper position against the eye.
Patients who return for a second or third thread lift to “refresh” the result accelerate this process dramatically. Each new thread adds fresh traction to an already compromised tendon. Ophthalmologic measurements on patients with two or more thread lifts reveal canthal angle drift of 8 to 12 millimeters — enough to create visible ectropion risk and chronic exposure keratopathy.

The 3-Year Point of No Return: What Happens When Tendon Separates From Bone
By month 30 to 36, the lateral canthal tendon has typically completed its detachment from the orbital rim. The consequences are severe and irreversible without surgical intervention. The eyelid rolls outward — this is ectropion. The inner surface of the eyelid, normally pressed gently against the eye, now faces outward, exposed to air, dust, and bacteria. Chronic conjunctivitis becomes routine. Corneal abrasions occur during sleep. Vision deteriorates from constant inflammation.
At this point, a simple canthoplasty — tightening the tendon — is useless because the tendon no longer exists as a functional structure. The patient requires a full canthal reconstruction: re-anchoring the lateral commissure to the orbital rim using tendon grafts, periosteal flaps, or temporalis fascia transfers. This procedure takes 3 to 4 hours under general anesthesia, demands an oculoplastic or specialized facial surgeon, and costs four to five times what the original thread lift cost.
The cruellest detail? Thread lift patients who reach this stage were almost universally told that thread lifts are “reversible,” “non-permanent,” or “dissolvable.” The thread itself dissolves. The damage it caused does not.
The Evidence: Ophthalmologic Data on Thread Lift Complications
Thread lift marketing relies on the absence of long-term follow-up data. Providers present their 30-day post-insertion photos and declare success. But ophthalmologic research measuring outcomes beyond the first year paints an entirely different picture.
A review of periorbital thread lift cases documented in oculoplastic literature reveals consistent patterns. Patients who received a single fox eye thread lift showed an average canthal angle drift of 4 to 6 millimeters at 12 months post-procedure. Patients who received two or more thread lifts in the same region showed drifts of 8 to 12 millimeters — well beyond the threshold for functional eyelid impairment. At that drift magnitude, the lower eyelid can no longer close fully during blinking, creating exposure dry eye and increasing ectropion risk by approximately 400 percent compared to unoperated controls.
The data also reveals an uncomfortable truth about repeat thread lifts. Many providers recommend “top-up” sessions when the initial lift settles, typically around 6 to 9 months. Each top-up adds fresh barbed sutures alongside the old ones, multiplying the mechanical load on the lateral canthal tendon. Patients who undergo three or more top-up sessions within two years show tendon detachment rates exceeding 60 percent, according to retrospective analyses from oculoplastic referral centers that receive these complication cases after the fact.
Canthopexy vs Canthoplasty: What Thread Providers Do Not Understand About Eyelid Mechanics
The confusion between canthopexy and canthoplasty runs deep — and thread lift providers exploit this confusion constantly. Understanding the difference is essential for grasping why the surgical approach used by SURGYTEAM’s Dr. MFO preserves the lateral canthal tendon while thread lifts destroy it.
Canthopexy reinforces the existing lateral canthal tendon without cutting it. The surgeon places a securing suture through the tendon and anchors it to the orbital rim periosteum, providing additional support while preserving the tendon’s natural insertion. The tendon continues to function. The eyelid continues to close properly. The anatomy remains intact.
Canthoplasty involves detaching the lateral canthal tendon, repositioning it, and reattaching it at a new location on the orbital rim. This is a stronger repositioning tool but sacrifices the original tendon insertion. It is appropriate in certain reconstructive scenarios but represents a more aggressive intervention.
Thread lifts do neither. They apply blind traction to a tendon they cannot see, through tissue planes they do not control, and leave the tendon to absorb forces it was never designed to handle. The comparison table below makes this contrast unmistakable.
| Factor | Thread Lift Fox Eye | Canthopexy-Based Fox Eye Surgery |
|---|---|---|
| Tendon Impact | Progressive stretching and detachment | Tendon reinforced and supported |
| Anatomical Control | Blind insertion, no direct visualization | Direct surgical visualization of tendon and rim |
| Force Distribution | Point loading on tendon by barbed suture | Broad loading across periosteal anchor |
| Scleral Show Risk | 8-12mm drift after 2+ threads | 1-2mm minimal drift, controlled |
| Ectropion Risk | High — progressive over 18-36 months | Low — tendon integrity preserved |
| Reversibility | Irreversible after tendon detachment | Revision possible through tendon adjustment |
| Longevity | 12-18 months aesthetic, permanent damage | Years of stable aesthetic result |
| Repeat Procedures | Accelerate tendon destruction | Not required — stable outcome |
| Cost of Correction (if damaged) | 4-5x original cost for canthal reconstruction | Covered within standard revision protocols |
How SURGYTEAM Dr. MFO Performs Canthopexy-Based Fox Eye Surgery
Dr. Mehmet Fatih Okyay — SURGYTEAM’s lead surgeon for facial contouring and periorbital surgery — takes a fundamentally different approach to fox eye surgery. Rather than blindly pulling the canthus with a thread, he performs an open canthopexy that directly visualizes and reinforces the lateral canthal tendon while achieving the desired aesthetic shape.
The procedure begins with a precise incision at the lateral canthal angle. Dr. MFO identifies the lateral canthal tendon under direct vision, confirming its integrity and insertion. He then places a permanent fixation suture through the tendon and anchors it to the periosteum of the lateral orbital rim at the exact position that achieves the patient’s desired canthal tilt. The tendon is supported — not destroyed. The eyelid closes fully. The anatomy remains functional.
This approach eliminates every risk that thread lifts introduce. There is no mechanical creep because the force is distributed across the broad periosteal anchor rather than a narrow barbed suture. There is no progressive tendon stretching because the tendon is reinforced, not loaded beyond its capacity. There is no countdown to irreversible damage because the procedure respects the tissue it operates on.
Dr. MFO’s FEBOPRAS certification and his specialization in periorbital surgery give him the precise credentials needed to assess thread-lift tendon damage and repair it before it becomes irreversible. Patients traveling for aesthetic surgery in Turkey benefit from his focused expertise in eyelid aesthetics — an area where generalist providers create damage and specialists prevent it.
The Tethering Risk Calculator: Has Your Thread Lift Already Caused Permanent Damage?
If you have had a fox eye thread lift, the following five questions will help determine whether canthal tethering has already begun causing irreversible damage to your lateral canthal tendon. Answer honestly — your eyelid function depends on it.
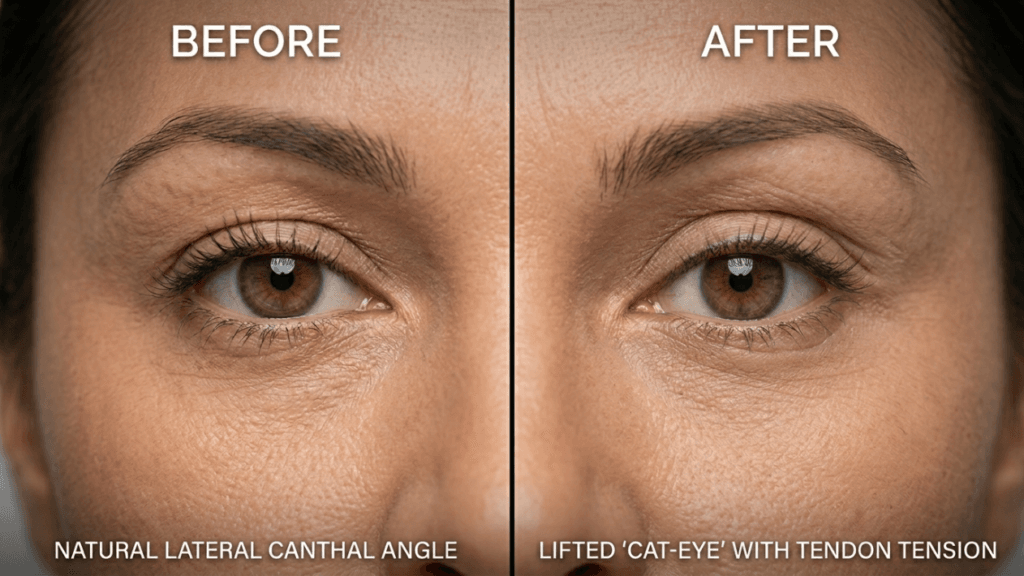
Question 1: Do You See More White Space at the Outer Corner of Your Eye Than Before Your Thread Lift?
Look closely in a mirror. Compare your current eye shape to pre-procedure photographs. If you see a visible gap between your iris and the outer corner — white sclera where none existed before — you have measurable scleral show. This indicates your canthal angle has drifted laterally. A drift of 3 millimeters or more suggests active tendon stretching. A drift exceeding 6 millimeters suggests partial detachment.
Question 2: Does Your Lower Eyelid Feel Loose or Shift When You Blink Firmly?
Pinch your lower eyelid gently between your thumb and forefinger. A healthy eyelid offers firm resistance and snaps back immediately. If your eyelid feels soft, stretches easily, or returns slowly to position, the lateral canthal tendon has lost its taut anchor. This is the lateral canthal distraction test — and a positive result suggests significant tendon damage.
Question 3: Have You Had Two or More Thread Lift Sessions?
Each additional thread lift compounds the mechanical load on your lateral canthal tendon. Patients with two or more thread lift sessions show 8 to 12 millimeters of canthal angle drift — the threshold where functional impairment begins. If you have had multiple sessions, your tendon is experiencing compounded traction that accelerates detachment significantly.
Question 4: Do You Experience Chronic Dryness, Tearing, or Grittiness in the Eye?
Your lower eyelid must sit flush against the globe to distribute tears evenly during blinking. When the canthal angle drifts outward, the lower eyelid separates from the eye surface, creating a gap. Tears pool incorrectly. The cornea dries between blinks. If you are using artificial tears more frequently since your thread lift, your eyelid mechanics have already been compromised.
Question 5: Has It Been More Than 18 Months Since Your First Thread Lift?
The tendon detachment timeline is relentless. At 18 months post-insertion, patients typically show early-to-moderate canthal drift even with a single thread. Beyond 30 months, the detachment rate accelerates sharply. If your first thread lift was over 18 months ago and you answered yes to any previous question, you need an urgent oculoplastic assessment — not another thread session.
Scoring: Zero yes answers indicates low current risk but warrants monitoring. One to two yes answers indicates moderate canthal tethering — seek evaluation within 3 months. Three or more yes answers indicates advanced canthal tethering with high probability of partial tendon detachment — seek immediate specialist consultation.

Fox Eye Surgery Done Right: The Surgical Alternative That Preserves Your Anatomy
Achieving the fox eye aesthetic does not require destroying your eyelid architecture. Surgical fox eye procedures — when performed by a specialist who understands periorbital anatomy — deliver superior aesthetic results with zero risk of canthal tethering, scleral show, or progressive ectropion.
The key distinction lies in how force is managed. Thread lifts apply continuous unidirectional traction through a foreign body anchored in soft tissue that shifts, settles, and degrades. Surgical fox eye surgery repositions the canthal angle through direct fixation to bone — the periosteum of the lateral orbital wall. Bone does not stretch. Bone does not creep. Bone does not detach under tension. The result is stable, predictable, and permanent.
Additionally, surgical approaches allow simultaneous upper blepharoplasty or brow lift procedures through the same incision. A patient receiving open canthopexy can address redundant upper eyelid skin, ptosis, or brow descent during a single operative session. Thread lifts cannot address any of these concerns — they merely pull at one angle and hope the tissue follows. Learn more about comprehensive eyelid procedures on our Blog.
What Canthal Reconstruction Involves When Threads Have Already Destroyed Your Tendon
For patients who have passed the point of no return, canthal reconstruction becomes necessary. This is not a quick fix. It is a complex reconstructive procedure that restores the lateral canthal tendon’s function using graft tissue and periosteal fixation techniques.
The surgeon identifies the remnant of the lateral canthal tendon — or what remains of it. If the tendon has completely detached and retracted, the surgeon harvests a tendon graft, typically from the temporalis fascia or a segment of the superior limb of the lateral canthal tendon. This graft bridges the gap between the lateral commissure and the orbital rim.
The graft is anchored to the periosteum of the lateral orbital wall using permanent sutures through drill holes in the bone or direct periosteal purchase. The position is calibrated precisely — too high creates scleral show, too low fails to correct the ectropion. The surgeon then closes the lateral canthal angle, creating a new commissure that matches the patient’s natural anatomy.
Recovery from canthal reconstruction takes 6 to 8 weeks. Swelling is significant. The eye may be patched for 48 to 72 hours. Patients require ophthalmologic monitoring for corneal health throughout recovery. The total cost — including surgeon fees, anesthesia, facility charges, and post-operative care — ranges from four to five times the original thread lift price.
Your 7-Step Action Plan: Protecting Your Eyelids Before the Countdown Hits Zero
If you have had a fox eye thread lift — or you are considering one — you need an immediate action plan. The clock on tendon damage starts the moment barbs engage your tissue. Follow these steps to protect your lateral canthal tendon from irreversible destruction.
- Assess your current canthal angle now. Take a photograph of your eyes in primary gaze and compare it to pre-procedure images. Measure any visible scleral show at the lateral corner. Anything beyond 2 millimeters requires professional evaluation.
- Perform the lateral canthal distraction test. Gently pull your lower eyelid away from the globe. If it moves more than 3 to 4 millimeters before meeting resistance, your tendon attachment has weakened. Document this finding.
- Calculate your tethering timeline. Count the months since your first thread lift. If you are past 18 months, your risk of progressive tendon detachment increases sharply. If you are past 30 months, urgency escalates dramatically — seek evaluation within weeks, not months.
- Stop all additional thread lift sessions immediately. Every top-up procedure accelerates tendon destruction. No provider should place additional traction on a tendon already under abnormal load. Refuse any “maintenance” thread procedures.
- Seek a specialist consultation with a FEBOPRAS-certified oculoplastic or facial surgeon. Only a surgeon with periorbital expertise can measure your canthal angle drift, assess tendon integrity, and determine whether damage is reversible. General practitioners and thread lift providers lack the training to diagnose canthal tethering.
- Request canthal angle photography and measurement. A qualified specialist will document your canthal angle, scleral show distance, and lower eyelid position using standardized clinical photography. These measurements serve as your baseline for monitoring progression or planning corrective surgery.
- Book a corrective canthopexy consultation before your window closes. If tendon damage is detected early, canthopexy can reinforce the tendon and prevent further drift. Once detachment is complete, only canthal reconstruction works — at dramatically higher cost, complexity, and recovery burden. Time is the decisive variable.
Your lateral canthal tendon is not a cosmetic accessory. It is a functional structure that protects your vision, maintains your tear film, and anchors your eyelid to your skull. Thread lifts treat it as an afterthought. Canthopexy-based surgery treats it as the critical structure it is. The difference between the two approaches determines whether you keep a beautiful, functional eye — or spend years managing a preventable deformity.
The Verdict: Thread Lifts Are a Ticking Clock on Your Eyelid Function
The fox eye thread lift industry has built its market on two claims: that the procedure is temporary and that it is reversible. Both claims are false in their implication. The thread dissolves — but the damage it inflicts on your lateral canthal tendon does not. The aesthetic result fades — but the mechanical creep, the tendon stretching, and the progressive detachment continue accumulating silently beneath the skin.
Patients who received thread lifts 18 to 36 months ago are now presenting to oculoplastic clinics with scleral show, ectropion, and tendon detachment that no simple procedure can reverse. These patients were never warned about canthal tethering because thread lift providers do not monitor outcomes beyond the first few weeks. By the time patients notice symptoms, the damage is often advanced.
The choice facing anyone who wants a fox eye aesthetic is straightforward. Thread lifts trade months of lifted appearance for years of progressive tendon destruction. Surgical fox eye procedures — particularly canthopexy-based approaches like those performed by SURGYTEAM’s Dr. MFO — deliver the same aesthetic outcome with structural integrity preserved. One approach burns down the bridge. The other reinforces it.
If you have had a thread lift, your 3-year countdown has already begun. The question is whether you act before it hits zero. Contact us at SURGYTEAM to schedule a canthopexy consultation with Dr. MFO — before reversible damage becomes irreversible deformity.
What is canthal tethering and why does it happen after a fox eye thread lift?
Canthal tethering is the progressive stretching and detachment of the lateral canthal tendon caused by continuous upward traction from barbed thread sutures. The thread applies force at an angle that does not match the tendon’s natural insertion, causing mechanical creep that slowly peels the tendon away from the orbital rim over 18 to 36 months.
How do I know if my thread lift has damaged my lateral canthal tendon?
Key warning signs include visible white sclera at the outer eye corner that was not present before your procedure, chronic dry eye or excessive tearing, a lower eyelid that feels loose when gently pulled, and progressive widening of the canthal angle over time. If you notice any of these symptoms, seek an oculoplastic evaluation immediately.
Why is canthopexy better than a thread lift for fox eye surgery?
Canthopexy reinforces the existing lateral canthal tendon by anchoring it directly to the periosteum of the orbital rim under surgical visualization. This preserves tendon function and distributes force across bone rather than soft tissue. Thread lifts apply blind traction that progressively stretches and detaches the tendon without any surgical control.
Can a damaged lateral canthal tendon be repaired?
Early tendon damage can often be addressed with canthopexy, which reinforces and stabilizes the tendon. However, once the tendon has fully detached from the orbital rim — typically after 30 to 36 months of thread lift traction — only a full canthal reconstruction using graft tissue and bone fixation can restore function. This procedure costs four to five times more than the original thread lift.
How long does canthopexy-based fox eye surgery last compared to a thread lift?
Canthopexy-based fox eye surgery provides a stable, permanent aesthetic result because the fixation is anchored to bone periosteum, which does not stretch or degrade under tension. Thread lifts typically lose their aesthetic effect within 12 to 18 months as the thread settles and tissue relaxes, while the underlying tendon damage continues to progress.
Who is qualified to assess thread lift damage to the lateral canthal tendon?
Only board-certified oculoplastic surgeons or specialized facial plastic surgeons with periorbital expertise can properly assess thread lift tendon damage. These specialists perform precise canthal angle measurements, evaluate lower eyelid position and tone, and determine whether canthal tethering has occurred. Thread lift providers and general practitioners lack this diagnostic capability.
What causes ectropion after fox eye thread lifts?
Ectropion occurs when the lateral canthal tendon detaches completely from the orbital rim, causing the lower eyelid to roll outward and lose contact with the eye surface. Thread lifts create this condition through progressive mechanical creep — the continuous upward traction slowly stretches the tendon beyond its elastic limit until it can no longer hold the eyelid in position.