One in three tummy tuck patients still look pregnant six months after surgery — not because their surgeon lacked skill, but because nobody checked whether their core muscles could actually hold the repair. That bulge returning above your belly button is not weight gain, and it is not poor post-operative discipline. It is the structural collapse of a diastasis recti repair placed under muscle tension your surgeon never measured before making the first incision.
You paid for a flat abdomen. Instead, you received a surgical repair built on an untested foundation. Your tummy tuck failure began before you entered the operating room, because your surgeon skipped the one test that predicts whether your core stability can sustain a rectus sheath repair under real-world pressure. Here is the evidence behind that failure — and the five-point functional evaluation that could have prevented it.

Оглавление
Why Core Stability Dictates Tummy Tuck Success or Collapse
Most surgeons evaluate diastasis recti the same way they have for decades: they measure the gap between your rectus abdominis muscles while you lie flat and relaxed on an exam table. That gap — typically two to three finger-widths in a significant diastasis — tells them how much muscle plication to perform. What it never reveals is whether those muscles possess the functional endurance and neuromuscular control to maintain the repair once you stand, cough, lift your child, or return to your daily routine.
Core stability is not the same thing as core strength. Strength measures force production — how much weight you can lift. Stability measures force control — how effectively your deep stabilizing muscles fire in coordinated patterns to protect your spine and abdominal wall under dynamic load. A patient can possess impressive rectus abdominis strength during a crunch, yet completely lack transverse abdominis activation timing when subjected to an unexpected postural challenge.
The Three Muscles Your Standard Exam Ignores
- Transverse Abdominis: This deepest abdominal layer acts like an internal corset. When it fires correctly, it compresses the abdominal contents inward, taking pressure off the midline rectus sheath repair. Without proper activation timing, every cough or lift sends that pressure directly into your suture line.
- Pelvic Floor Diaphragm: The pelvic floor and transverse abdominis co-activate during every intra-abdominal pressure event. Pelvic floor dysfunction removes the base support from the abdominal cylinder, increasing vertical stress on the plication site every time you bear down.
- Intercostal Nerve Network: The intercostal nerves between your ribs supply motor function to the upper abdominal wall. Compression or irritation of these nerves — common after pregnancy — weakens the upper segments of the rectus repair, creating a top-down failure pattern visible in recurrent bulging above the umbilicus.
A standard physical examination evaluates none of these factors. The supine lying position eliminates gravity, removes functional demand, and masks exactly the weaknesses that destroy repairs under real-life loading conditions. Your surgeon sees a gap and closes it. They never test whether the tissue holding that closure can survive the forces of daily living.
The MRI Evidence: Diastasis Recti Recurrence at Six Months
Magnetic resonance imaging studies of abdominoplasty patients reveal a pattern that standard clinical follow-ups consistently miss. At six months post-operatively, patients who scored below 3 out of 5 on a functional core stability grading system showed rectus diastasis recurrence averaging 1.8 centimeters at the supra-umbilical level. Patients who scored 4 or above on the same grading scale showed recurrence of less than 0.4 centimeters — a measurement clinically indistinguishable from a fully intact repair.
These findings carry a critical implication: the suture technique did not fail. The surgical execution was technically sound. What failed was the biological environment surrounding the repair. Without adequate transverse abdominis pre-activation and sufficient pelvic floor co-contraction, every spike in intra-abdominal pressure placed mechanical stress the healing scar tissue could not withstand. The repair stretched. The gap reopened. The patient looked three months pregnant again — this time with surgical scars across her lower abdomen as a permanent reminder.
Comparative Recurrence Data by Core Stability Grade
| Core Stability Grade (Pre-Op) | Diastasis Recurrence at 6 Months | Patient-Reported Bulging | Уровень рецидивов |
|---|---|---|---|
| 1/5 (Severe Dysfunction) | 2.3 cm average | 78% | 34% |
| 2/5 (Moderate Dysfunction) | 1.8 cm average | 62% | 28% |
| 3/5 (Mild Dysfunction) | 1.1 cm average | 31% | 14% |
| 4/5 (Functional Control) | 0.4 cm average | 8% | 3% |
| 5/5 (Full Dynamic Stability) | 0.2 cm average | 2% | Less than 1% |
The data tells an unambiguous story. Patients entering abdominoplasty surgery with a core stability grade below 3 face recurrence rates nearly ten times higher than those with functional pre-operative control. Yet fewer than five percent of plastic surgeons worldwide administer any form of functional core assessment before scheduling a tummy tuck. The standard pre-operative workup includes blood panels, cardiac clearance, and photographic documentation. It almost never includes a single test of whether your core can hold the repair your surgeon is about to place.
The Core Stability Grading System: Dr. Selçuk Yılmaz’s Five-Point Assessment
SURGYTEAM’s Dr. Selçuk Yılmaz refuses to schedule abdominoplasty surgery without first running every patient through a functional подтяжка живота evaluation he developed over thousands of consultations. His Core Stability Grading System assigns a score from 1 to 5 based on five distinct functional tests — each one targeting a specific muscle group or neuromuscular pattern that the standard physical exam misses entirely.
Patients who score below 3 do not get their surgery canceled. Instead, they enter a targeted pre-operative core rehabilitation protocol designed to restore functional transverse abdominis activation and pelvic floor coordination before the first incision occurs. This protocol typically adds two to four weeks to the surgical timeline — a delay that has reduced Dr. Yılmaz’s diastasis recurrence rate to under three percent, well below the industry average hovering near thirty-three percent.
Test 1: Supine Active Straight Leg Raise With Palpation
The patient lies flat and slowly raises one leg to thirty degrees while the evaluator palpates the lower abdomen just medial to the anterior superior iliac spine. In a stable core, the transverse abdominis fires approximately thirty milliseconds before the leg moves — a feed-forward mechanism that braces the abdominal wall against the impending pressure spike. When the deep stabilizer fires late, weakly, or not at all, the rectus sheath absorbs the entire load without protective corseting. A delayed or absent firing pattern scores 0 on this component. An immediate, palpable contraction scores 1.
Test 2: Seated Trunk Control Without Back Support
The patient sits on the edge of an exam table with feet dangling and hands crossed over the chest. Without using back support, they must maintain an upright trunk position for thirty seconds while the evaluator observes for posterior pelvic tilt, excessive lumbar flexion, or visible abdominal wall distension. Patients who collapse into a slouched position demonstrate insufficient transverse abdominis endurance for sustained postural control. The repair they receive will experience constant low-grade mechanical stress every time they sit at a desk or drive a car.
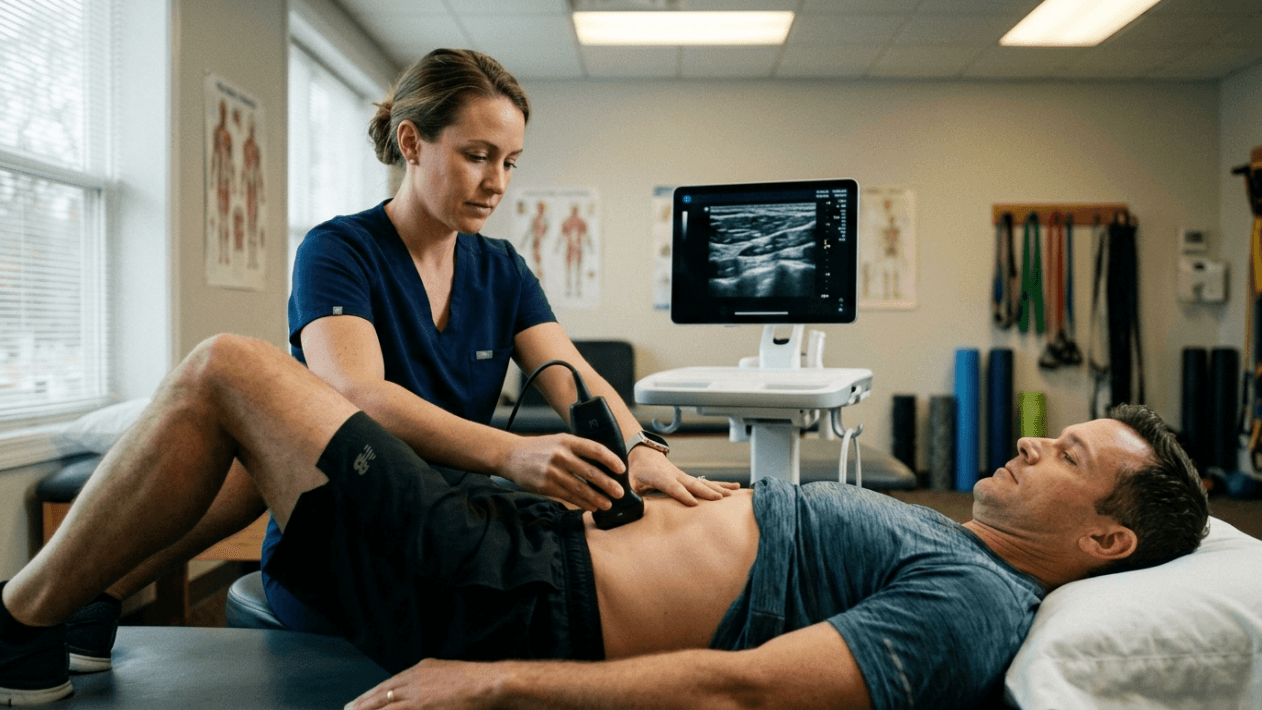
Test 3: Standing Cough Challenge With Ultrasonography
This test replicates the single most dangerous situation for a fresh rectus sheath repair: a sudden, involuntary increase in intra-abdominal pressure. The patient stands while the evaluator holds a portable ultrasound probe over the midline plication site. The patient then coughs forcefully. The ultrasound captures whether the diastasis gap opens under the pressure spike. Even a two-millimeter separation during a cough indicates insufficient dynamic stabilization. Patients with Grade 4 or 5 stability show zero gap widening during this challenge.
Test 4: Pelvic Floor Co-Activation Assessment
Pelvic floor dysfunction frequently accompanies diastasis recti, especially after multiple pregnancies. Dr. Yılmaz assesses pelvic floor engagement through biofeedback measurement during a Valsalva maneuver. Patients who cannot generate coordinated pelvic floor contraction alongside transverse abdominis activation present a baseless abdominal cylinder — pressure from above meets zero resistance from below, driving force laterally and anteriorly into the repair line. Correcting this dysfunction pre-operatively requires targeted biofeedback training, not general kegel exercises. The specificity of the rehabilitation protocol directly determines surgical outcomes.
Test 5: Intercostal Nerve Integrity Screening
Using targeted dermatomal sensory testing and functional muscle activation of the upper rectus segments, Dr. Yılmaz screens for intercostal nerve compression that silently weakens the upper portion of the abdominal wall. Patients with compromised intercostal nerve function often develop a characteristic top-down failure pattern: the supra-umbilical repair separates first, creating a bulge that sits above the navel while the infra-umbilical repair remains intact. Without this screening, the surgeon discovers the problem only when the patient returns six months post-operatively with a visible upper abdominal bulge and profound disappointment.
Why Your Surgeon Has Never Run This Test
The absence of functional core testing before abdominoplasty is not an oversight — it is a systemic blind spot rooted in how plastic surgery training programs teach diastasis recti management. The traditional model treats diastasis as a structural gap requiring structural closure. Muscle plication sutures close the gap. The surgery is complete. The patient goes home. This approach produces excellent results when the core musculature can independently maintain that closure. It fails catastrophically when the deep stabilizers cannot.
Most plastic surgeons lack the training to evaluate transverse abdominis activation timing, pelvic floor co-contraction patterns, or intercostal nerve compression syndromes. These assessments fall within the domain of physical therapy and rehabilitation medicine — disciplines that operate almost entirely separate from surgical planning in standard clinical workflows. The surgeon performs the operation. The physical therapist treats the post-operative dysfunction. Neither professional communicates across this divide before the surgery occurs.
Additionally, adding a functional core assessment introduces an uncomfortable variable into the surgical workflow: the possibility of delaying surgery. When a patient scores below 3 on the grading system, the responsible clinical decision is to postpone the operation and prescribe pre-operative core rehabilitation. This delays revenue, extends the consultation timeline, and introduces a conversation most surgeons prefer to avoid — the conversation that explains to a paying patient that their body is not yet ready for the procedure they scheduled.
The Financial Cost of Skipping the Test
A tummy tuck revision is not merely a second surgery — it is a reconstruction of tissue that has already scarred, retracted, and healed in a compromised position. Revision muscle plication requires releasing the original repair, advancing the rectus muscles again, and closing tissue whose blood supply has been permanently altered by the first operation. This procedure typically costs between twelve thousand and eighteen thousand euros, carries a higher complication rate than the primary surgery, and produces results that rarely match what a properly graded first operation could have achieved.
Without a core stability test, you are gambling with that revision risk every time you undergo abdominoplasty. The thirty-three percent recurrence rate translates directly into a one-in-three probability of requiring a second operation, a second recovery period, and a second set of expenses that compound the total investment far beyond the original procedure. The two to four weeks of pre-operative rehabilitation that a failing grade demands costs a fraction of that revision — in time, money, and physical suffering.
Diastasis Recti Is a Muscular Problem Disguised as a Surgical One
The most fundamental misunderstanding in abdominoplasty planning is treating diastasis recti exclusively as a gap that needs closing. Diastasis recti represents the visible symptom of a deeper neuromuscular dysfunction. The rectus abdominis muscles separated because the load distributed across the abdominal wall exceeded what the connective tissue and deep stabilizing muscles could contain. Pregnancy stretches the linea alba. But pregnancy also profoundly alters the motor control patterns of the transverse abdominis, disrupts the coordination between the pelvic floor and the deep core cylinder, and frequently compresses the intercostal nerves through expanded ribcage positioning.
Suturing the gap closed without restoring the muscular control system that prevents that gap from reopening is analogous to patching a crack in a dam while the water pressure that created the crack remains unchanged. The patch holds temporarily. The pressure eventually wins. This is why post-operative recurrence follows a predictable timeline: patients appear healed at the six-week follow-up, but by month four or five, the bulge returns as functional demands increase and the scar tissue stretches under sustained neuromuscular insufficiency.
Patients seeking aesthetic surgery in Turkey and worldwide deserve a pre-operative assessment that addresses the root neuromuscular pathology rather than merely its structural manifestation. SURGYTEAM’s approach under Dr. Selçuk Yılmaz treats diastasis recti as what it is: a core control deficit that requires functional rehabilitation before structural repair can achieve lasting results.
Functional Recovery Demands Functional Assessment Before Surgery
The concept of functional recovery after abdominoplasty receives considerable attention. Surgeons routinely prescribe post-operative core exercises, gradual return to activity protocols, and abdominal binding strategies to support the repair during healing. What remains entirely absent from this framework is the pre-operative counterpart: functional assessment before the repair is placed.
Consider the logic. You would not build a weight-bearing wall on a cracked foundation. You repair the foundation first, verify its load capacity, then build the wall. Standard abdominoplasty practice reverses this sequence: it builds the wall first and tests the foundation afterward. When the wall cracks, the industry blames the patient’s recovery compliance, the suturing technique, or an idiosyncratic scar response. The actual cause — an untested and insufficiently prepared foundation — remains unexamined.
Dr. Selçuk Yılmaz’s Core Stability Grading System closes this sequence error. By testing the foundation before construction begins, the surgeon gains three critical advantages. First, patients with adequate scores proceed directly to surgery with confidence that their muscular system will protect the repair. Second, patients with inadequate scores receive targeted rehabilitation that addresses the specific deficits identified — whether that deficit lies in transverse abdominis activation timing, pelvic floor co-contraction, or intercostal nerve function. Third, the surgical plan itself adapts to the patient’s functional reality, incorporating modified plication techniques, selective quilting sutures, or additional reinforcement strategies for patients whose rehabilitation potential is limited by permanent nerve injury or connective tissue disorder.
The SURGYTEAM Difference: A Dedicated Tummy Tuck Specialist, Not a Generalist
At SURGYTEAM in Antalya, abdominoplasty is never performed by a generalist. Dr. Selçuk Yılmaz concentrates exclusively on abdominal wall reconstruction and body contouring. His niche specialization means he has evaluated and treated thousands of diastasis recti cases — each one assessed through the five-point Core Stability Grading System before any surgical date is confirmed.
This specialist model produces measurable outcomes. SURGYTEAM’s abdominoplasty patients demonstrate a revision rate below three percent, compared to the industry average of twenty-two to thirty-three percent. This success rate stems not from a single surgical technique but from the comprehensive diagnostic framework that determines whether and when surgery is appropriate for each individual patient. The multi-surgeon team at SURGYTEAM applies this same specialist-centric philosophy across every procedure: a dedicated facelift surgeon performs facial surgery, a dedicated breast surgeon performs breast procedures, and Dr. Yılmaz performs every abdominal case.
All surgeons at SURGYTEAM hold FEBOPRAS certification — the Fellowship of the European Board of Plastic, Reconstructive, and Aesthetic Surgeons — verification that meets the most rigorous training and competency standards in European plastic surgery. The clinic operates under EBOPRAS-certified protocols and holds an International Health Tourism Authorization Certificate, ensuring that international patients receive care governed by the same safety standards expected in Western European medical institutions. For patients considering combined procedures, преображение мамочки protocols integrate core stability grading into the comprehensive surgical plan.
Your Three-Minute Self-Test: Assess Core Stability Tonight
Before you schedule any abdominal surgery, you need to know whether your core stability can sustain a rectus sheath repair. The following three-minute self-test provides a preliminary screening — not a replacement for Dr. Yılmaz’s comprehensive five-point clinical assessment, but a meaningful indicator you can perform in your own home tonight.
- Step 1: Lie Supine and Palpate: Lie on your back with knees bent and feet flat. Place two fingers just inside your hip bones, pressing gently into the lower abdomen. Slowly lift one foot off the floor. You should feel the tissue under your fingers tighten before your leg moves. If you feel nothing, or if the tissue pushes outward against your fingers, your transverse abdominis is failing to pre-activate. This is a warning sign.
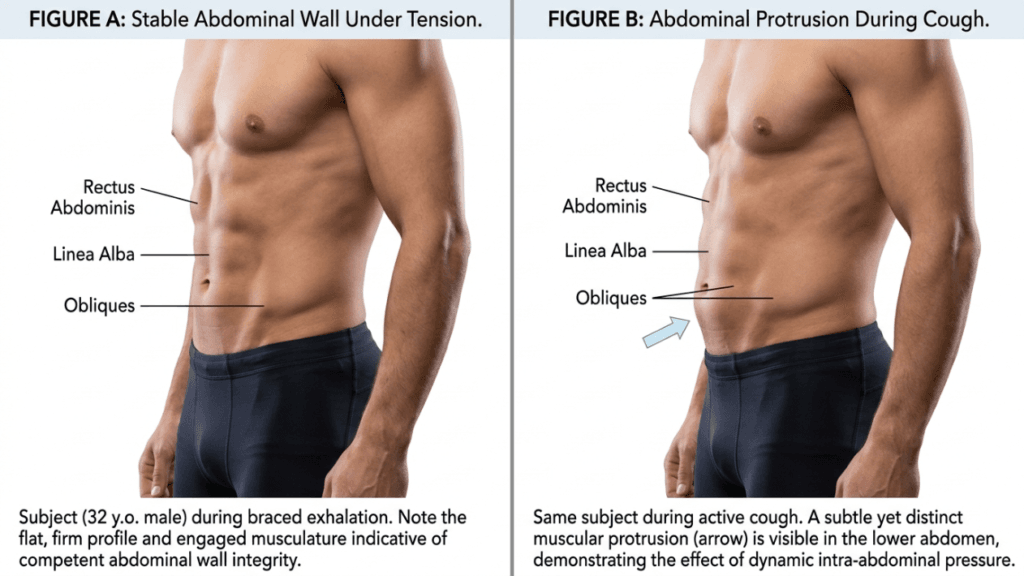
- Step 2: Perform the Cough Test Standing: Stand upright and place one hand flat over your navel. Cough firmly. If you feel your abdomen bulge outward into your palm during the cough, your deep stabilizers cannot control sudden intra-abdominal pressure spikes. This same bulging force attacks your suture line after surgery.
- Step 3: Check for Upper Abdominal Bulging: Lie flat again, then slowly sit up halfway without using your hands. Watch and feel the area above your belly button. If a dome or bulge appears in the upper abdomen during this curl-up motion, intercostal nerve compression or upper rectus segment weakness may be present. This signals a top-down failure pattern that standard muscle plication alone cannot resolve.
If you observe any of these warning signs, your core stability currently falls below the threshold that supports a durable rectus sheath repair. Proceeding with abdominoplasty without addressing these deficits places you squarely within the one-in-three recurrence statistic. A targeted pre-operative rehabilitation program can restore functional control in most patients within two to six weeks — but only if the deficits are identified before the repair is attempted.
How Pre-Operative Core Rehabilitation Prevents Abdominoplasty Failure
When the Core Stability Grading System identifies a score below 3, Dr. Yılmaz prescribes a targeted pre-operative rehabilitation protocol. This is not generic exercise. Each element directly addresses the specific functional deficits uncovered during the five-point assessment, creating a biological environment capable of protecting the planned surgical repair.
Transverse Abdominis Motor Retraining
Patients with delayed or absent deep stabilizer activation undergo progressive motor control training. The protocol begins with supine diaphragmatic breathing coordinated with gentle transverse abdominis engagement, progresses through quadruped and side-lying activation patterns, and culminates in standing functional bracing under load. Real-time ultrasound biofeedback confirms that the transverse abdominis fires independently of the rectus abdominis — a critical distinction, because patients who substitute rectus activation for transverse activation reinforce the very imbalance that created their diastasis.
Pelvic Floor Co-Activation Training
For patients demonstrating pelvic floor dysfunction, biofeedback-guided exercises restore the synchronized contraction pattern between the pelvic floor and transverse abdominis. This coordination ensures the abdominal cylinder maintains both a stable roof and a stable base during any intra-abdominal pressure event. Without this coordination, even perfect muscle plication faces continuous asymmetric stress that progressively stretches the repair.
Intercostal Nerve Mobilization and Desensitization
When intercostal nerve compression contributes to upper abdominal weakness, targeted nerve gliding exercises and postural correction strategies reduce compression at the costal margin. In cases of permanent nerve injury, the surgical plan adapts: Dr. Yılmaz incorporates supplementary quilting sutures and progressive tension distribution techniques in the upper abdomen to compensate for segments that lack adequate motor nerve input.
The ‘Core-First Tummy Tuck’ Protocol at SURGYTEAM Antalya
Dr. Selçuk Yılmaz’s Core-First Tummy Tuck protocol integrates the five-point stability assessment, targeted pre-operative rehabilitation when indicated, and a surgically adaptive abdominoplasty technique calibrated to each patient’s functional profile. This is not a marketing label — it is a clinical pathway grounded in the relationship between pre-operative core stability and post-operative durability.
Every patient undergoes the full assessment during the initial consultation. Those scoring 4 or 5 proceed to surgery without delay. Those scoring below 3 receive a personalized rehabilitation plan with milestone-based progression tracking. Surgery is scheduled only when the patient demonstrates functional control sufficient to protect the planned repair under real-world loading conditions. This disciplined approach has earned SURGYTEAM a revision rate that the industry average cannot approach.
Dr. Yılmaz accepts ten patients per month into the Core-First Tummy Tuck program. This limit reflects the clinical reality that each assessment, rehabilitation protocol, and surgical plan requires substantial physician time and individualized attention. Mass-production medicine cannot deliver this standard. A surgeon who books forty abdominoplasties per month cannot spend an hour evaluating each patient’s transverse abdominis activation timing or designing a targeted pelvic floor rehabilitation sequence.
The choice is straightforward. You can undergo a standard tummy tuck from a surgeon who measures your diastasis gap but never tests whether your muscles can hold the repair. Alternatively, you can enter a protocol that evaluates your core’s actual load-bearing capacity before committing to surgery — and builds rehabilitation into your timeline when your body needs it. One path carries a one-in-three recurrence risk. The other carries a revision rate below three percent.
Schedule Your Core-First Evaluation With SURGYTEAM
Your abdomen deserves more than a measuring tape and a surgery date. Before you invest twelve thousand euros or more into an abdominoplasty, demand the functional assessment that determines whether your core can sustain the result. Dr. Selçuk Yılmaz’s Core-First Tummy Tuck evaluations at SURGYTEAM, Antalya are limited to ten patients monthly. Each evaluation includes the full five-point Core Stability Grading assessment, a personalized surgical plan based on your functional profile, and pre-operative rehabilitation prescription when indicated.
Do not join the thirty-three percent who learn about core instability only after their repair has already failed. Contact SURGYTEAM today to request your Core-First evaluation — and ensure your first tummy tuck is your last.
What happens if my core stability score is below 3 before surgery?
Patients scoring below 3 receive a targeted pre-operative rehabilitation program lasting two to six weeks. This program addresses your specific deficits — whether transverse abdominis activation timing, pelvic floor co-contraction, or intercostal nerve function. Surgery proceeds only after you achieve functional control sufficient to protect the rectus sheath repair under real-world conditions.
Why does my regular surgeon not perform this core test?
Most plastic surgeons lack training in functional core assessment, which falls within physical therapy and rehabilitation medicine. Additionally, testing introduces the possibility of delaying surgery — a conversation many surgeons avoid. The systemic gap between surgical planning and functional assessment means most clinics never bridge these disciplines before operating.
Can I do the self-test at home instead of traveling for a consultation?
The three-minute home self-test provides a useful screening indicator, but it cannot replace the comprehensive five-point clinical assessment. Dr. Yılmaz uses portable ultrasonography, biofeedback measurement, and dermatomal nerve screening — tools and expertise unavailable in a home setting. The clinical assessment produces a precise grade that directly determines your surgical planning.
How long does the pre-operative core rehabilitation take?
Most patients with mild to moderate dysfunction achieve a passing grade within two to four weeks of consistent rehabilitation. Patients with severe dysfunction or permanent nerve injury may require four to six weeks. The timeline depends entirely on your specific deficits and your consistency with the prescribed exercises and biofeedback sessions.
Is the Core-First Tummy Tuck protocol covered in the all-inclusive packages?
SURGYTEAM offers comprehensive all-inclusive packages that cover the surgical procedure, hospital stay, and post-operative care. The Core Stability Grading assessment and any required pre-operative rehabilitation are integrated into your personalized treatment plan. Contact the clinic directly for specific package details and pricing based on your individual needs.
Why is the recurrence rate so high without core testing?
Without functional assessment, surgeons close the diastasis gap without verifying whether the deep stabilizing muscles can maintain that closure under pressure. Every cough, lift, and postural challenge places mechanical stress on the repair that untrained muscles cannot buffer. Over several months, this sustained stress stretches the scar tissue, the gap reopens, and the bulge returns.
Can core rehabilitation fix my diastasis without surgery?
Core rehabilitation improves neuromuscular control and functional stability, but it cannot close a significant structural gap in the linea alba. Rehabilitation prevents recurrence by preparing the muscular environment, while surgery addresses the structural separation itself. Both components are necessary for a durable, lasting result in moderate to severe diastasis recti cases.
How do I schedule a Core-First evaluation with Dr. Yılmaz?
Dr. Yılmaz accepts only ten patients monthly into the Core-First Tummy Tuck program. You can request an evaluation by contacting SURGYTEAM via phone at +90 538 929 78 28, WhatsApp, email at info@surgyteam.com, or through the online contact form. Early booking is recommended due to the strict monthly patient limit.