Ein von drei Patienten nach einer Bauchstraffung sieht sechs Monate nach der Operation noch schwanger aus – nicht weil der Chirurg ungeschickt war, sondern weil niemand überprüft hat, ob die Kernmuskulatur die Reparatur tatsächlich halten kann. Die Wölbung über dem Bauchnabel ist keine Gewichtszunahme und keine mangelnde postoperative Disziplin. Es ist der strukturelle Kollaps einer Diastasis‑Recti‑Reparatur, die unter Muskelspannung steht, die Ihr Chirurg vor dem ersten Schnitt nie gemessen hat.
Sie haben für einen flachen Bauch bezahlt. Stattdessen erhielten Sie eine chirurgische Reparatur, die auf einem ungetesteten Fundament gebaut ist. Ihr Bauchstraffungs‑Fehlschlag begann, bevor Sie den Operationssaal betraten, weil Ihr Chirurg den einen Test übersprungen hat, der vorhersagt, ob Ihre Kernstabilität eine Rektus‑Sheath‑Reparatur unter realen Druckbedingungen tragen kann. Hier ist die Evidenz hinter diesem Fehlschlag – und die fünf‑Punkte‑Funktionsbewertung, die ihn hätte verhindern können.

Inhaltsverzeichnis
Warum Kernstabilität den Erfolg oder das Scheitern einer Bauchstraffung bestimmt
Die meisten Chirurgen beurteilen Diastasis recti seit Jahrzehnten auf dieselbe Weise: Sie messen die Lücke zwischen Ihren geraden Bauchmuskeln, während Sie flach und entspannt auf einer Untersuchungsliege liegen. Diese Lücke – typischerweise zwei bis drei Fingerbreiten bei einer signifikanten Diastase – gibt ihnen an, wie viel Muskelplättchen sie durchführen müssen. Was sie nie erkennen, ist, ob diese Muskeln die funktionelle Ausdauer und neuromuskuläre Kontrolle besitzen, um die Reparatur zu erhalten, wenn Sie stehen, husten, Ihr Kind heben oder zu Ihrer täglichen Routine zurückkehren.
Kernstabilität ist nicht dasselbe wie Kernkraft. Kraft misst die Kraftproduktion – wie viel Gewicht Sie heben können. Stabilität misst die Kraftkontrolle – wie effektiv Ihre tiefen stabilisierenden Muskeln in koordinierten Mustern feuern, um Ihre Wirbelsäule und Bauchwand bei dynamischer Belastung zu schützen. Ein Patient kann beeindruckende Stärke des geraden Bauchmuskels bei einem Crunch besitzen, jedoch völlig das Timing der Aktivierung des transversen Abdominis bei einer unerwarteten Haltungsherausforderung fehlen.
Die drei Muskeln, die Ihre Standarduntersuchung ignoriert
- Transversus Abdominis: Diese tiefste Bauchschicht wirkt wie ein innerer Korsett. Wenn sie korrekt feuert, komprimiert sie die Bauchorgane nach innen und nimmt den Druck von der mittleren Rektus-Scheiden‑Reparatur. Ohne richtiges Aktivierungs‑Timing führt jeder Husten oder Heben diesen Druck direkt in Ihre Nahtlinie.
- Beckenboden‑Zwerchfell: Der Beckenboden und der transversus abdominis aktivieren sich gemeinsam bei jedem intraabdominalen Druckereignis. Eine Beckenbodendysfunktion entfernt die Basisunterstützung vom Bauchzylinder und erhöht den vertikalen Stress an der Plättchenstelle jedes Mal, wenn Sie Druck ausüben.
- Interkostales Nervennetz: Die interkostalen Nerven zwischen Ihren Rippen versorgen die obere Bauchwand mit motorischer Funktion. Eine Kompression oder Reizung dieser Nerven – häufig nach einer Schwangerschaft – schwächt die oberen Segmente der Rektus‑Reparatur und erzeugt ein von oben nach unten verlaufendes Versagensmuster, das bei wiederholtem Vorwölben über dem Bauchnabel sichtbar wird.
Eine Standard‑körperliche Untersuchung bewertet keinen dieser Faktoren. Die liegende Rückenlage eliminiert die Schwerkraft, entfernt funktionelle Anforderungen und verdeckt genau die Schwächen, die Reparaturen unter realen Belastungsbedingungen zerstören. Ihr Chirurg sieht eine Lücke und schließt sie. Sie testen nie, ob das Gewebe, das diese Schließung hält, den Kräften des Alltags standhalten kann.
Der MRT‑Nachweis: Wiederauftreten von Diastasis Recti nach sechs Monaten
Magnetresonanztomographie‑Studien von Abdominoplastik‑Patienten zeigen ein Muster, das standardmäßige klinische Nachuntersuchungen konsequent übersehen. Sechs Monate postoperativ zeigten Patienten, die im funktionellen Kernstabilitäts‑Bewertungssystem weniger als 3 von 5 Punkten erzielten, ein Wiederauftreten der Rektus‑Diastase mit durchschnittlich 1,8 cm auf supra‑umbilikaler Ebene. Patienten, die 4 oder mehr Punkte auf derselben Skala erzielten, zeigten ein Wiederauftreten von weniger als 0,4 cm – eine Messung, die klinisch nicht von einer vollständig intakten Reparatur zu unterscheiden ist.
Diese Ergebnisse haben eine kritische Implikation: Die Nahttechnik ist nicht versagt. Die chirurgische Ausführung war technisch einwandfrei. Was versagte, war das biologische Umfeld um die Reparatur herum. Ohne ausreichende Voraktivierung des transversen Abdominis und ausreichende Co‑Kontraktion des Beckenbodens setzte jeder Druckspike im intraabdominalen Raum mechanischen Stress auf das heilende Narbengewebe, den es nicht standhalten konnte. Die Reparatur dehnte sich. Die Lücke öffnete sich wieder. Die Patientin sah wieder aus wie drei Monate schwanger – diesmal mit chirurgischen Narben über ihrem Unterbauch als dauerhafte Erinnerung.
Vergleichende Rezidivdaten nach Kernstabilitätsgrad
| Kernstabilitätsgrad (prä‑operativ) | Diastase‑Wiederauftreten nach 6 Monaten | Patientenberichtete Vorwölbung | Revisionsrate |
|---|---|---|---|
| 1/5 (Schwere Funktionsstörung) | Durchschnittlich 2,3 cm | 78% | 34% |
| 2/5 (Mäßige Funktionsstörung) | Durchschnittlich 1,8 cm | 62% | 28% |
| 3/5 (Leichte Dysfunktion) | Durchschnittlich 1,1 cm | 31% | 14% |
| 4/5 (Funktionelle Kontrolle) | Durchschnittlich 0,4 cm | 8% | 3% |
| 5/5 (Vollständige dynamische Stabilität) | Durchschnittlich 0,2 cm | 2% | Weniger als 1% |
Die Daten erzählen eine eindeutige Geschichte. Patienten, die mit einem Core-Stabilitätsgrad unter 3 in die Bauchdeckenstraffung gehen, haben fast zehnmal höhere Rückfallraten als diejenigen mit funktioneller präoperativer Kontrolle. Dennoch führen weniger als fünf Prozent der plastischen Chirurgen weltweit irgendeine Form der funktionellen Core-Bewertung vor der Planung einer Bauchdeckenstraffung durch. Der Standard‑Pre‑Op‑Check umfasst Bluttests, kardiologische Freigabe und fotografische Dokumentation. Ein Test, ob Ihr Core die geplante Reparatur halten kann, ist fast nie enthalten.
Das Kernstabilitäts‑Bewertungssystem: Dr. Selçuk Yılmaz’ Fünf‑Punkte‑Assessment
SURGYTEAMs Dr. Selçuk Yılmaz verweigert die Terminvereinbarung für eine Bauchdeckenstraffung, ohne zuerst jeden Patienten durch eine funktionelle Bauchstraffung Bewertung zu führen, die er über tausende Konsultationen entwickelt hat. Sein Core-Stability‑Grading‑System vergibt eine Punktzahl von 1 bis 5 basierend auf fünf unterschiedlichen funktionellen Tests – jeder zielt auf eine spezifische Muskelgruppe oder ein neuromuskuläres Muster ab, das die Standard‑körperliche Untersuchung völlig verfehlt.
Patienten, die unter 3 Punkte erzielen, erhalten nicht die Absage der Operation. Stattdessen beginnen sie ein gezieltes präoperatives Core‑Rehabilitationsprotokoll, das die funktionelle Aktivierung des transversus abdominis und die Koordination des Beckenbodens wiederherstellt, bevor der erste Schnitt gesetzt wird. Dieses Protokoll verlängert den Operationszeitplan typischerweise um zwei bis vier Wochen – eine Verzögerung, die die Rückfallrate von Dr. Yılmaz auf unter drei Prozent gesenkt hat, weit unter dem Branchendurchschnitt von etwa dreiunddreißig Prozent.
Test 1: Supine aktive gestreckte Beinhebung mit Palpation
Der Patient liegt flach und hebt langsam ein Bein auf dreißig Grad, während der Prüfer den Unterbauch medial zur vorderen oberen Darmbeinstachel abtastet. Bei stabilem Core feuert der transversus abdominis etwa dreißig Millisekunden bevor das Bein bewegt wird – ein feed‑forward‑Mechanismus, der die Bauchwand gegen den bevorstehenden Druckanstieg abstützt. Wenn der tiefe Stabilisator zu spät, schwach oder gar nicht feuert, absorbiert die Rektusschicht die gesamte Last ohne schützendes Korsett. Ein verspätetes oder fehlendes Feuerbild erhält 0 Punkte für diese Komponente. Eine sofortige, tastbare Kontraktion erhält 1 Punkt.
Test 2: Sitzende Rumpfkontrolle ohne Rückenstütze
Der Patient sitzt am Rand eines Untersuchungstisches, die Füße baumeln und die Hände über der Brust gekreuzt. Ohne Rückenstütze muss er für dreißig Sekunden eine aufrechte Rumpfposition halten, während der Prüfer auf hintere Beckenneigung, übermäßige Lendenflexion oder sichtbare Bauchwanddistension achtet. Patienten, die in eine gekrümmte Haltung zusammenbrechen, zeigen unzureichende Ausdauer des transversus abdominis für anhaltende Haltungskontrolle. Die Reparatur, die sie erhalten, wird bei jedem Sitzen am Schreibtisch oder Fahren eines Autos ständiger, leichter mechanischer Belastung ausgesetzt sein.
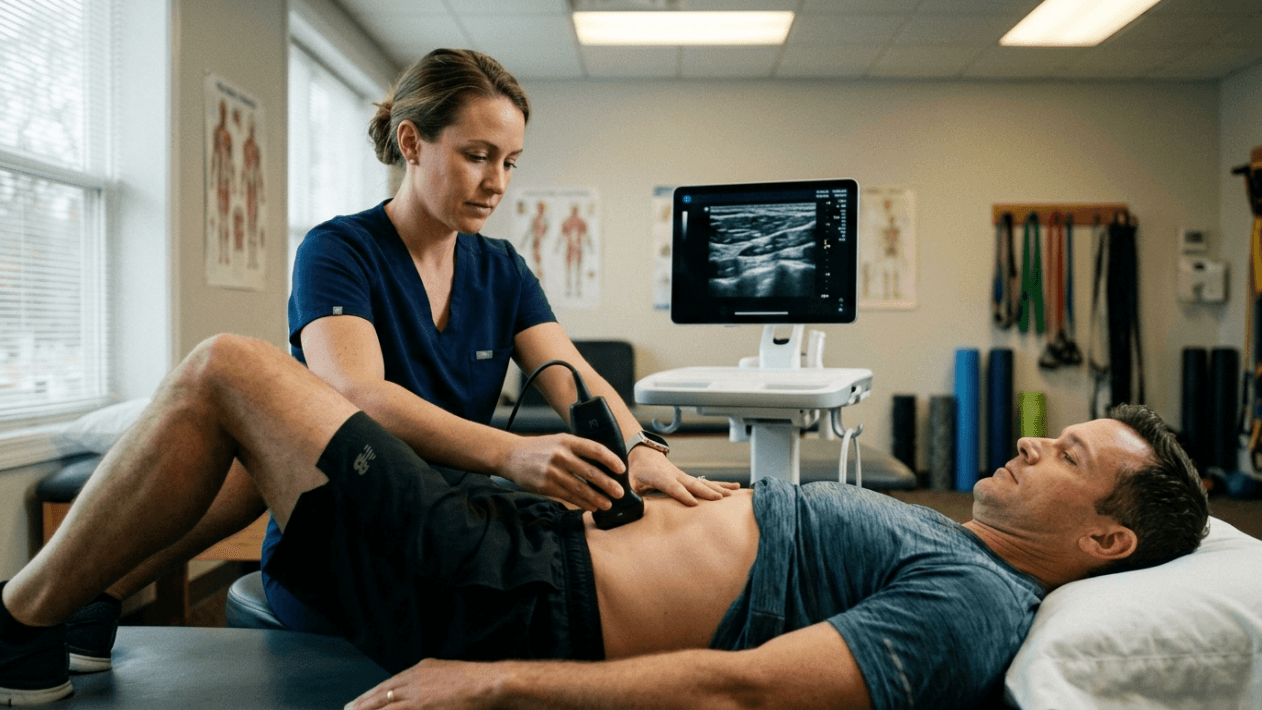
Test 3: Stehende Husten‑Herausforderung mit Ultraschall
Dieser Test reproduziert die gefährlichste Situation für eine frische Rektusschichtreparatur: einen plötzlichen, unwillkürlichen Anstieg des intraabdominalen Drucks. Der Patient steht, während der Prüfer einen tragbaren Ultraschallkopf über der mittleren Plikationsstelle hält. Der Patient hustet dann kräftig. Der Ultraschall erfasst, ob die Diastase‑Lücke beim Druckanstieg öffnet. Bereits eine zweimillimeter‑Trennung beim Husten weist auf unzureichende dynamische Stabilisierung hin. Patienten mit Grad‑4‑ oder Grad‑5‑Stabilität zeigen während dieser Herausforderung keinerlei Lückenerweiterung.
Test 4: Beckenboden‑Koaktivierungs‑Bewertung
Pelvic floor dysfunction frequently accompanies diastasis recti, especially after multiple pregnancies. Dr. Yılmaz assesses pelvic floor engagement through biofeedback measurement during a Valsalva maneuver. Patients who cannot generate coordinated pelvic floor contraction alongside transverse abdominis activation present a baseless abdominal cylinder — pressure from above meets zero resistance from below, driving force laterally and anteriorly into the repair line. Correcting this dysfunction pre-operatively requires targeted biofeedback training, not general kegel exercises. The specificity of the rehabilitation protocol directly determines surgical outcomes.
Test 5: Screening der Integrität der Interkostalnerven
Using targeted dermatomal sensory testing and functional muscle activation of the upper rectus segments, Dr. Yılmaz screens for intercostal nerve compression that silently weakens the upper portion of the abdominal wall. Patients with compromised intercostal nerve function often develop a characteristic top-down failure pattern: the supra-umbilical repair separates first, creating a bulge that sits above the navel while the infra-umbilical repair remains intact. Without this screening, the surgeon discovers the problem only when the patient returns six months post-operatively with a visible upper abdominal bulge and profound disappointment.
Warum Ihr Chirurg diesen Test nie durchgeführt hat
The absence of functional core testing before abdominoplasty is not an oversight — it is a systemic blind spot rooted in how plastic surgery training programs teach diastasis recti management. The traditional model treats diastasis as a structural gap requiring structural closure. Muscle plication sutures close the gap. The surgery is complete. The patient goes home. This approach produces excellent results when the core musculature can independently maintain that closure. It fails catastrophically when the deep stabilizers cannot.
Most plastic surgeons lack the training to evaluate transverse abdominis activation timing, pelvic floor co-contraction patterns, or intercostal nerve compression syndromes. These assessments fall within the domain of physical therapy and rehabilitation medicine — disciplines that operate almost entirely separate from surgical planning in standard clinical workflows. The surgeon performs the operation. The physical therapist treats the post-operative dysfunction. Neither professional communicates across this divide before the surgery occurs.
Additionally, adding a functional core assessment introduces an uncomfortable variable into the surgical workflow: the possibility of delaying surgery. When a patient scores below 3 on the grading system, the responsible clinical decision is to postpone the operation and prescribe pre-operative core rehabilitation. This delays revenue, extends the consultation timeline, and introduces a conversation most surgeons prefer to avoid — the conversation that explains to a paying patient that their body is not yet ready for the procedure they scheduled.
Die finanziellen Kosten des Überspringens des Tests
A tummy tuck revision is not merely a second surgery — it is a reconstruction of tissue that has already scarred, retracted, and healed in a compromised position. Revision muscle plication requires releasing the original repair, advancing the rectus muscles again, and closing tissue whose blood supply has been permanently altered by the first operation. This procedure typically costs between twelve thousand and eighteen thousand euros, carries a higher complication rate than the primary surgery, and produces results that rarely match what a properly graded first operation could have achieved.
Without a core stability test, you are gambling with that revision risk every time you undergo abdominoplasty. The thirty-three percent recurrence rate translates directly into a one-in-three probability of requiring a second operation, a second recovery period, and a second set of expenses that compound the total investment far beyond the original procedure. The two to four weeks of pre-operative rehabilitation that a failing grade demands costs a fraction of that revision — in time, money, and physical suffering.
Diastasis Recti ist ein muskuläres Problem, das als chirurgisches dargestellt wird
The most fundamental misunderstanding in abdominoplasty planning is treating diastasis recti exclusively as a gap that needs closing. Diastasis recti represents the visible symptom of a deeper neuromuscular dysfunction. The rectus abdominis muscles separated because the load distributed across the abdominal wall exceeded what the connective tissue and deep stabilizing muscles could contain. Pregnancy stretches the linea alba. But pregnancy also profoundly alters the motor control patterns of the transverse abdominis, disrupts the coordination between the pelvic floor and the deep core cylinder, and frequently compresses the intercostal nerves through expanded ribcage positioning.
Suturing the gap closed without restoring the muscular control system that prevents that gap from reopening is analogous to patching a crack in a dam while the water pressure that created the crack remains unchanged. The patch holds temporarily. The pressure eventually wins. This is why post-operative recurrence follows a predictable timeline: patients appear healed at the six-week follow-up, but by month four or five, the bulge returns as functional demands increase and the scar tissue stretches under sustained neuromuscular insufficiency.
Patients seeking ästhetische Eingriffe in die Türkei reisen and worldwide deserve a pre-operative assessment that addresses the root neuromuscular pathology rather than merely its structural manifestation. SURGYTEAM’s approach under Dr. Selçuk Yılmaz treats diastasis recti as what it is: a core control deficit that requires functional rehabilitation before structural repair can achieve lasting results.
Funktionelle Genesung erfordert funktionelle Bewertung vor der Operation
The concept of functional recovery after abdominoplasty receives considerable attention. Surgeons routinely prescribe post-operative core exercises, gradual return to activity protocols, and abdominal binding strategies to support the repair during healing. What remains entirely absent from this framework is the pre-operative counterpart: functional assessment before the repair is placed.
Consider the logic. You would not build a weight-bearing wall on a cracked foundation. You repair the foundation first, verify its load capacity, then build the wall. Standard abdominoplasty practice reverses this sequence: it builds the wall first and tests the foundation afterward. When the wall cracks, the industry blames the patient’s recovery compliance, the suturing technique, or an idiosyncratic scar response. The actual cause — an untested and insufficiently prepared foundation — remains unexamined.
Dr. Selçuk Yılmaz’s Core Stability Grading System closes this sequence error. By testing the foundation before construction begins, the surgeon gains three critical advantages. First, patients with adequate scores proceed directly to surgery with confidence that their muscular system will protect the repair. Second, patients with inadequate scores receive targeted rehabilitation that addresses the specific deficits identified — whether that deficit lies in transverse abdominis activation timing, pelvic floor co-contraction, or intercostal nerve function. Third, the surgical plan itself adapts to the patient’s functional reality, incorporating modified plication techniques, selective quilting sutures, or additional reinforcement strategies for patients whose rehabilitation potential is limited by permanent nerve injury or connective tissue disorder.
Der SURGYTEAM Unterschied: Ein spezialisierter Bauchstraffungs-Experte, kein Generalist
Bei SURGYTEAM in Antalya wird eine Bauchdeckenstraffung niemals von einem Allgemeinmediziner durchgeführt. Dr. Selçuk Yılmaz konzentriert sich ausschließlich auf die Rekonstruktion der Bauchwand und die Körperkonturierung. Seine Nischenspezialisierung bedeutet, dass er Tausende von Diastasis‑Recti‑Fällen evaluiert und behandelt hat – jeder Fall wurde anhand des fünf‑stufigen Core‑Stability‑Bewertungssystems beurteilt, bevor ein Operationstermin bestätigt wurde.
Dieses Facharztmodell liefert messbare Ergebnisse. Die Bauchdeckenstraffungs‑Patienten von SURGYTEAM zeigen eine Revisionsrate von unter drei Prozent, verglichen mit dem Branchendurchschnitt von zweiundzwanzig bis dreiunddreißig Prozent. Diese Erfolgsrate resultiert nicht aus einer einzigen Operationstechnik, sondern aus dem umfassenden diagnostischen Rahmen, der bestimmt, ob und wann eine Operation für den einzelnen Patienten angemessen ist. Das Mehr‑Chirurgen‑Team von SURGYTEAM wendet dieselbe fachärztlich‑zentrierte Philosophie bei jedem Eingriff an: ein dedizierter Facelifting‑Chirurg führt Gesichtsoperationen durch, ein dedizierter Brustchirurg führt Brustverfahren durch, und Dr. Yılmaz führt jeden Bauchfall durch.
Alle Chirurgen bei SURGYTEAM besitzen die FEBOPRAS‑Zertifizierung – das Fellowship of the European Board of Plastic, Reconstructive, and Aesthetic Surgeons – ein Nachweis, der den strengsten Ausbildungs‑ und Kompetenzstandards in der europäischen plastischen Chirurgie entspricht. Die Klinik arbeitet nach EBOPRAS‑zertifizierten Protokollen und besitzt ein Internationales Gesundheits‑Tourismus‑Genehmigungszertifikat, das sicherstellt, dass internationale Patienten eine Versorgung erhalten, die den gleichen Sicherheitsstandards entspricht, die in westeuropäischen medizinischen Einrichtungen erwartet werden. Für Patienten, die kombinierte Eingriffe in Erwägung ziehen, Mama-Makeover integrieren die Protokolle die Core‑Stability‑Bewertung in den umfassenden Operationsplan.
Ihr dreiminütiger Selbsttest: Kernstabilität heute Abend prüfen
Bevor Sie eine Bauchoperation planen, müssen Sie wissen, ob Ihre Core‑Stability eine Reparatur der Rectus‑Sheath‑Schicht tragen kann. Der folgende dreiminütige Selbsttest bietet ein vorläufiges Screening – keinen Ersatz für Dr. Yılmaz’ umfassende fünf‑stufige klinische Bewertung, aber einen sinnvollen Indikator, den Sie heute Abend zu Hause durchführen können.
- Step 1: Lie Supine and Palpate: Lie on your back with knees bent and feet flat. Place two fingers just inside your hip bones, pressing gently into the lower abdomen. Slowly lift one foot off the floor. You should feel the tissue under your fingers tighten before your leg moves. If you feel nothing, or if the tissue pushes outward against your fingers, your transverse abdominis is failing to pre-activate. This is a warning sign.
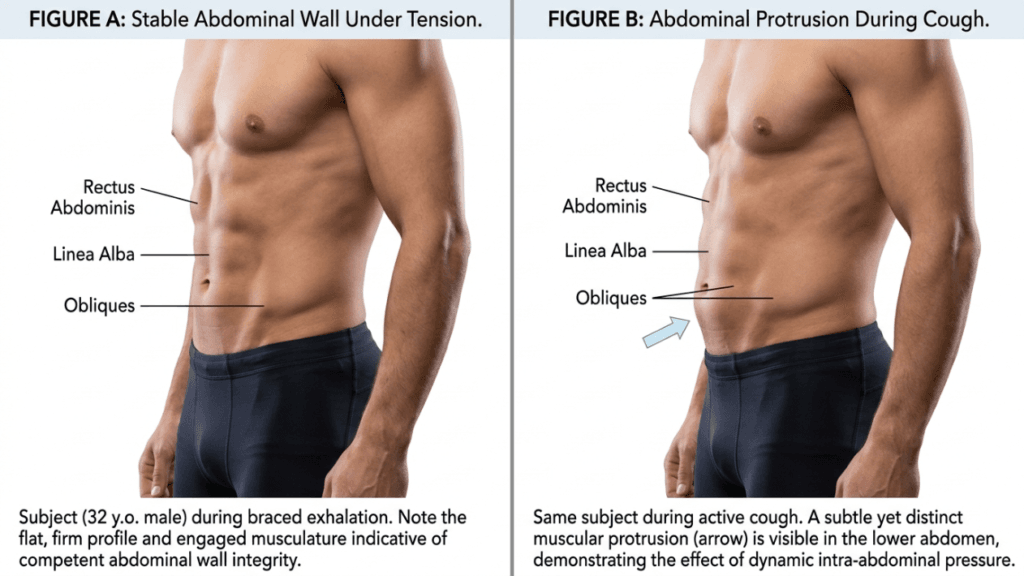
- Step 2: Perform the Cough Test Standing: Stand upright and place one hand flat over your navel. Cough firmly. If you feel your abdomen bulge outward into your palm during the cough, your deep stabilizers cannot control sudden intra-abdominal pressure spikes. This same bulging force attacks your suture line after surgery.
- Step 3: Check for Upper Abdominal Bulging: Lie flat again, then slowly sit up halfway without using your hands. Watch and feel the area above your belly button. If a dome or bulge appears in the upper abdomen during this curl-up motion, intercostal nerve compression or upper rectus segment weakness may be present. This signals a top-down failure pattern that standard muscle plication alone cannot resolve.
If you observe any of these warning signs, your core stability currently falls below the threshold that supports a durable rectus sheath repair. Proceeding with abdominoplasty without addressing these deficits places you squarely within the one-in-three recurrence statistic. A targeted pre-operative rehabilitation program can restore functional control in most patients within two to six weeks — but only if the deficits are identified before the repair is attempted.
Wie präoperative Kernrehabilitation das Scheitern einer Abdominoplastik verhindert
When the Core Stability Grading System identifies a score below 3, Dr. Yılmaz prescribes a targeted pre-operative rehabilitation protocol. This is not generic exercise. Each element directly addresses the specific functional deficits uncovered during the five-point assessment, creating a biological environment capable of protecting the planned surgical repair.
Motorisches Retraining des transversus abdominis
Patients with delayed or absent deep stabilizer activation undergo progressive motor control training. The protocol begins with supine diaphragmatic breathing coordinated with gentle transverse abdominis engagement, progresses through quadruped and side-lying activation patterns, and culminates in standing functional bracing under load. Real-time ultrasound biofeedback confirms that the transverse abdominis fires independently of the rectus abdominis — a critical distinction, because patients who substitute rectus activation for transverse activation reinforce the very imbalance that created their diastasis.
Koaktivierungstraining des Beckenbodens
For patients demonstrating pelvic floor dysfunction, biofeedback-guided exercises restore the synchronized contraction pattern between the pelvic floor and transverse abdominis. This coordination ensures the abdominal cylinder maintains both a stable roof and a stable base during any intra-abdominal pressure event. Without this coordination, even perfect muscle plication faces continuous asymmetric stress that progressively stretches the repair.
Mobilisierung und Desensibilisierung des Interkostalnervs
When intercostal nerve compression contributes to upper abdominal weakness, targeted nerve gliding exercises and postural correction strategies reduce compression at the costal margin. In cases of permanent nerve injury, the surgical plan adapts: Dr. Yılmaz incorporates supplementary quilting sutures and progressive tension distribution techniques in the upper abdomen to compensate for segments that lack adequate motor nerve input.
Das ‘Core-First Tummy Tuck’‑Protokoll bei SURGYTEAM Antalya
Dr. Selçuk Yılmaz’s Core-First Tummy Tuck protocol integrates the five-point stability assessment, targeted pre-operative rehabilitation when indicated, and a surgically adaptive abdominoplasty technique calibrated to each patient’s functional profile. This is not a marketing label — it is a clinical pathway grounded in the relationship between pre-operative core stability and post-operative durability.
Every patient undergoes the full assessment during the initial consultation. Those scoring 4 or 5 proceed to surgery without delay. Those scoring below 3 receive a personalized rehabilitation plan with milestone-based progression tracking. Surgery is scheduled only when the patient demonstrates functional control sufficient to protect the planned repair under real-world loading conditions. This disciplined approach has earned SURGYTEAM a revision rate that the industry average cannot approach.
Dr. Yılmaz accepts ten patients per month into the Core-First Tummy Tuck program. This limit reflects the clinical reality that each assessment, rehabilitation protocol, and surgical plan requires substantial physician time and individualized attention. Mass-production medicine cannot deliver this standard. A surgeon who books forty abdominoplasties per month cannot spend an hour evaluating each patient’s transverse abdominis activation timing or designing a targeted pelvic floor rehabilitation sequence.
The choice is straightforward. You can undergo a standard tummy tuck from a surgeon who measures your diastasis gap but never tests whether your muscles can hold the repair. Alternatively, you can enter a protocol that evaluates your core’s actual load-bearing capacity before committing to surgery — and builds rehabilitation into your timeline when your body needs it. One path carries a one-in-three recurrence risk. The other carries a revision rate below three percent.
Vereinbaren Sie Ihre Core-First‑Bewertung mit SURGYTEAM
Your abdomen deserves more than a measuring tape and a surgery date. Before you invest twelve thousand euros or more into an abdominoplasty, demand the functional assessment that determines whether your core can sustain the result. Dr. Selçuk Yılmaz’s Core-First Tummy Tuck evaluations at SURGYTEAM, Antalya are limited to ten patients monthly. Each evaluation includes the full five-point Core Stability Grading assessment, a personalized surgical plan based on your functional profile, and pre-operative rehabilitation prescription when indicated.
Do not join the thirty-three percent who learn about core instability only after their repair has already failed. Contact SURGYTEAM today to request your Core-First evaluation — and ensure your first tummy tuck is your last.
Was passiert, wenn mein Kernstabilitätsscore vor der Operation unter 3 liegt?
Patients scoring below 3 receive a targeted pre-operative rehabilitation program lasting two to six weeks. This program addresses your specific deficits — whether transverse abdominis activation timing, pelvic floor co-contraction, or intercostal nerve function. Surgery proceeds only after you achieve functional control sufficient to protect the rectus sheath repair under real-world conditions.
Warum führt mein regulärer Chirurg diesen Kern-Test nicht durch?
Most plastic surgeons lack training in functional core assessment, which falls within physical therapy and rehabilitation medicine. Additionally, testing introduces the possibility of delaying surgery — a conversation many surgeons avoid. The systemic gap between surgical planning and functional assessment means most clinics never bridge these disciplines before operating.
Kann ich den Selbsttest zu Hause machen, anstatt für eine Beratung zu reisen?
The three-minute home self-test provides a useful screening indicator, but it cannot replace the comprehensive five-point clinical assessment. Dr. Yılmaz uses portable ultrasonography, biofeedback measurement, and dermatomal nerve screening — tools and expertise unavailable in a home setting. The clinical assessment produces a precise grade that directly determines your surgical planning.
Wie lange dauert die präoperative Kernrehabilitation?
Most patients with mild to moderate dysfunction achieve a passing grade within two to four weeks of consistent rehabilitation. Patients with severe dysfunction or permanent nerve injury may require four to six weeks. The timeline depends entirely on your specific deficits and your consistency with the prescribed exercises and biofeedback sessions.
Ist das Core-First‑Bauchstraffungs‑Protokoll in den All‑Inclusive‑Paketen enthalten?
SURGYTEAM offers comprehensive all-inclusive packages that cover the surgical procedure, hospital stay, and post-operative care. The Core Stability Grading assessment and any required pre-operative rehabilitation are integrated into your personalized treatment plan. Contact the clinic directly for specific package details and pricing based on your individual needs.
Warum ist die Rückfallrate ohne Core-Testing so hoch?
Without functional assessment, surgeons close the diastasis gap without verifying whether the deep stabilizing muscles can maintain that closure under pressure. Every cough, lift, and postural challenge places mechanical stress on the repair that untrained muscles cannot buffer. Over several months, this sustained stress stretches the scar tissue, the gap reopens, and the bulge returns.
Kann Kernrehabilitation meine Diastase ohne Operation beheben?
Core rehabilitation improves neuromuscular control and functional stability, but it cannot close a significant structural gap in the linea alba. Rehabilitation prevents recurrence by preparing the muscular environment, while surgery addresses the structural separation itself. Both components are necessary for a durable, lasting result in moderate to severe diastasis recti cases.
Wie vereinbare ich eine Core-First‑Bewertung bei Dr. Yılmaz?
Dr. Yılmaz accepts only ten patients monthly into the Core-First Tummy Tuck program. You can request an evaluation by contacting SURGYTEAM via phone at +90 538 929 78 28, WhatsApp, email at info@surgyteam.com, or through the online contact form. Early booking is recommended due to the strict monthly patient limit.